

Home-based motor imagery intervention improves functional performance following total knee arthroplasty in the short term: a randomized controlled trial
- PMID: 33008432
- PMCID: PMC7531130
- DOI: 10.1186/s13018-020-01964-4
Home-based motor imagery intervention improves functional performance following total knee arthroplasty in the short term: a randomized controlled trial
Abstract
Background: Motor imagery (MI) is effective in improving motor performance in the healthy asymptomatic adult population. However, its possible effects among older orthopaedic patients are still poorly investigated. Therefore, this study explored whether the addition of motor imagery to routine physical therapy reduces the deterioration of quadriceps muscle strength and voluntary activation (VA) as well as other variables related to motor performance in patients after total knee arthroplasty (TKA).
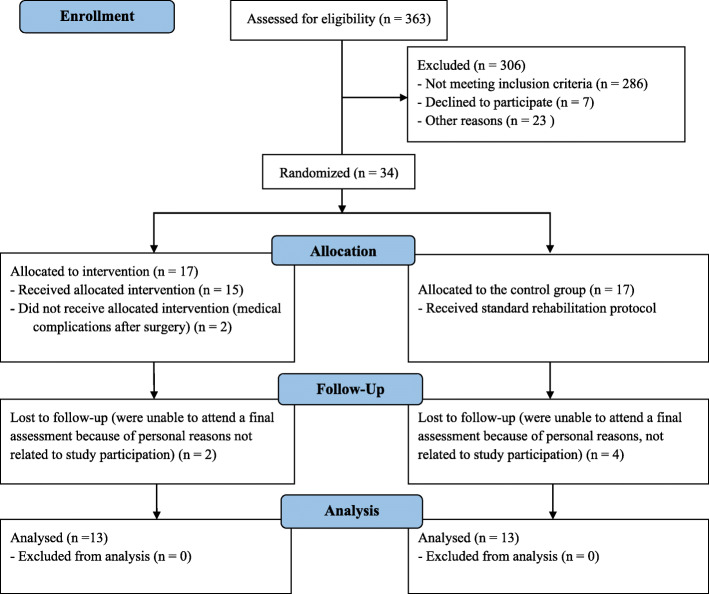
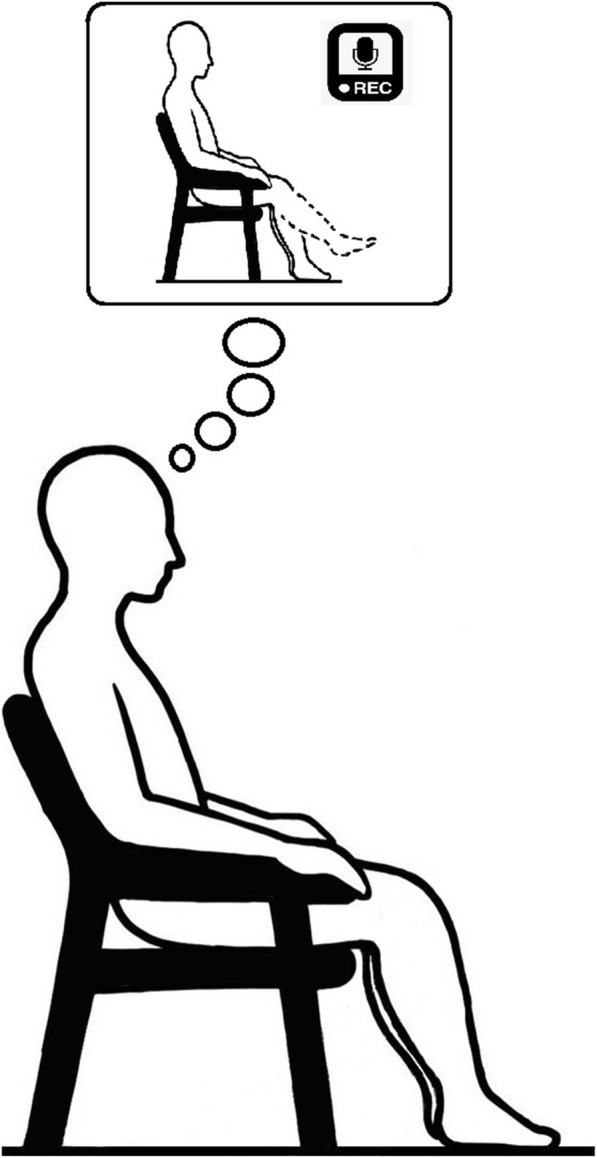
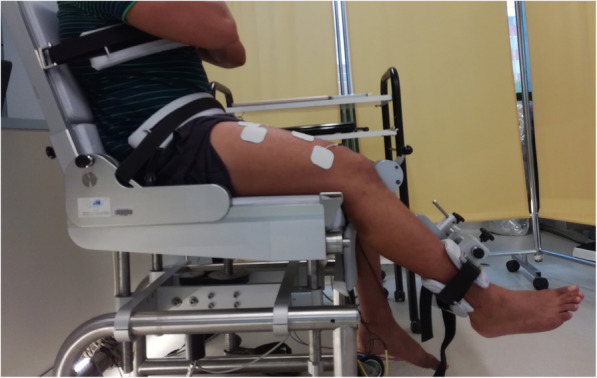
Methods: Twenty-six patients scheduled for TKA were randomized to either MI practice combined with routine physical therapy group (MIp) or to a control group receiving physical therapy alone (CON). MIp consisted of maximal voluntary isometric contraction (MViC) task: 15 min/day in the hospital, then 5 times/week in their homes for 4 weeks. MViC and VA of quadriceps muscle, knee flexion and extension range of motion, pain level, along with a Timed Up-and-Go Test (TUG) and self-reported measure of physical function (assessed using the Oxford Knee Score questionnaire [OKS]) were evaluated before (PRE) and 1 month after surgery (POST).
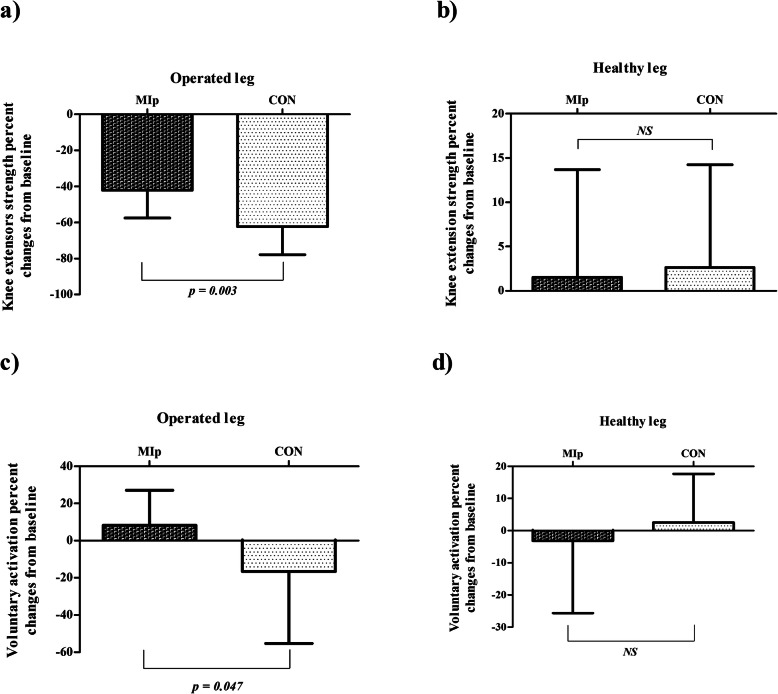
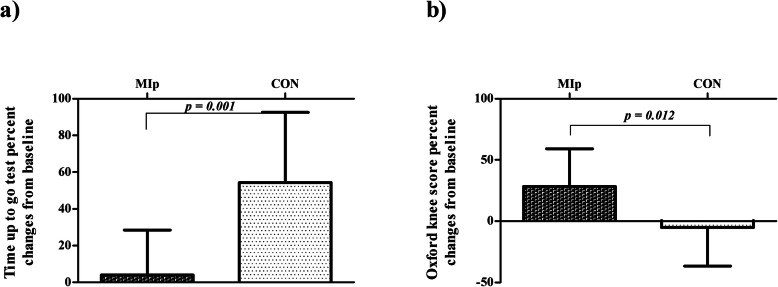
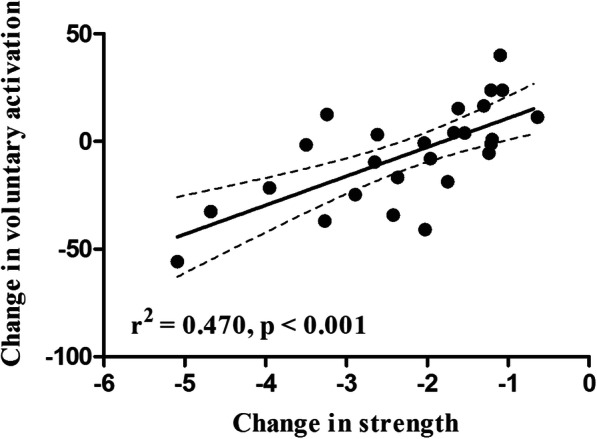
Results: Significantly better rehabilitation outcomes were evident on the operated leg for the MIp group compared to CON: at POST, the MIp showed lower strength decrease (p = 0.012, η2 = 0.237) and unaltered VA, significantly greater than CON (p = 0.014, η2 = 0.227). There were no significant differences in knee flexion and extension range of motion and pain level (p > 0.05). Further, MIp patients performed better in TUG (p < 0.001, η2 = 0.471) and reported better OKS scores (p = 0.005, η2 = 0.280). The non-operated leg showed no significant differences in any outcomes at POST (all p > 0.05). In addition, multiple linear regression analysis showed that failure of voluntary activation explained 47% of the quadriceps muscle strength loss, with no significant difference in perceived level of pain.
Conclusion: MI practice, when added to physical therapy, improves both objective and subjective measures of patients' physical function after TKA, and facilitates transfer of MI strength task on functional mobility.
Trial registration: Retrospectively registered on ClinicalTrials.gov NCT03684148.
Keywords: Cognitive training; Knee osteoarthritis; Mental simulation; Muscle activation; Physical function; Rehabilitation; Total knee replacement.
Conflict of interest statement
The authors declare that they have no conflict of interest relevant to the content of this article.
Funding
The present study was a part of a PhD project, thus it was partly supported by the Slovenian Research Agency (ARRS).
Figures
References
-
- Bourne R. Remains of the day: Outcome measurements in total knee arthroplasty. Orthopedics. 2000;23:995–998. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
