

Cardiac-MRI Predicts Clinical Worsening and Mortality in Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis
- PMID: 33008758
- PMCID: PMC7525356
- DOI: 10.1016/j.jcmg.2020.08.013
Cardiac-MRI Predicts Clinical Worsening and Mortality in Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis
Erratum in
-
Correction.JACC Cardiovasc Imaging. 2021 Apr;14(4):884. doi: 10.1016/j.jcmg.2021.02.001. JACC Cardiovasc Imaging. 2021. PMID: 33832670 Free PMC article. No abstract available.
Abstract
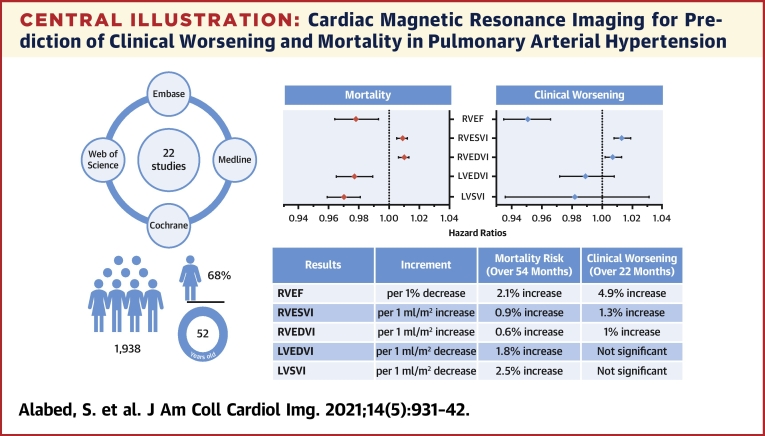
Objectives: This meta-analysis evaluates assessment of pulmonary arterial hypertension (PAH), with a focus on clinical worsening and mortality.
Background: Cardiac magnetic resonance (CMR) has prognostic value in the assessment of patients with PAH. However, there are limited data on the prediction of clinical worsening, an important composite endpoint used in PAH therapy trials.
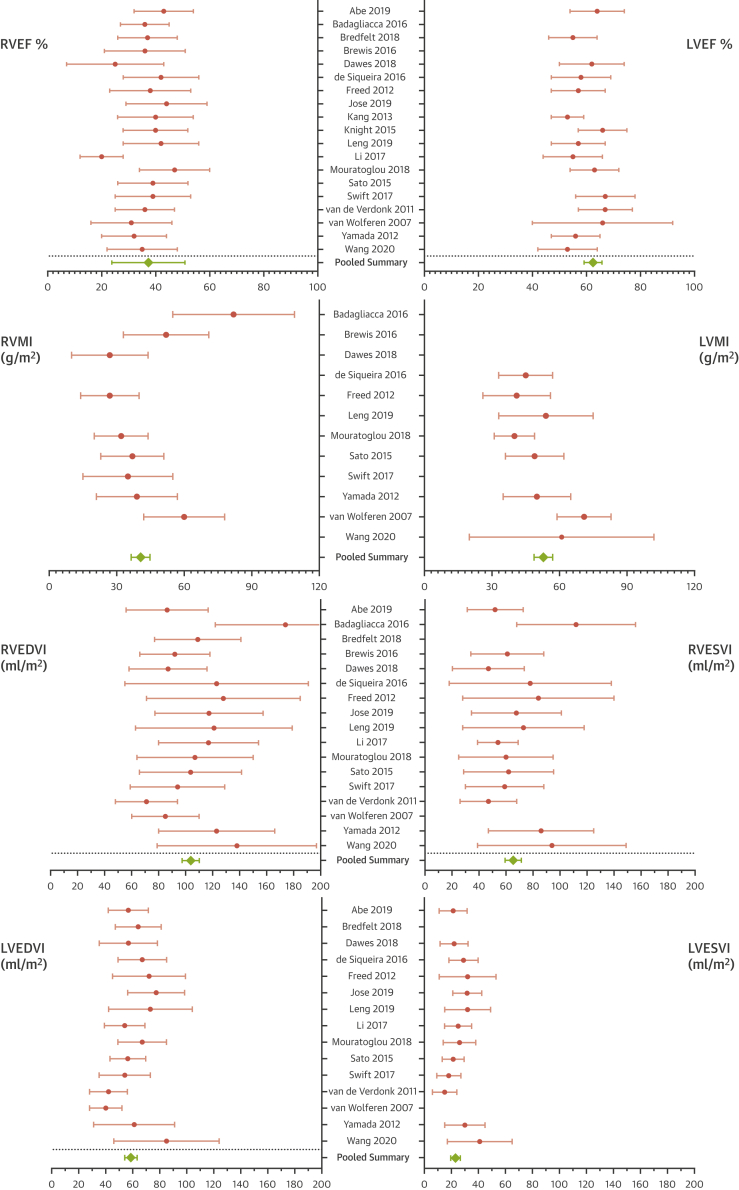
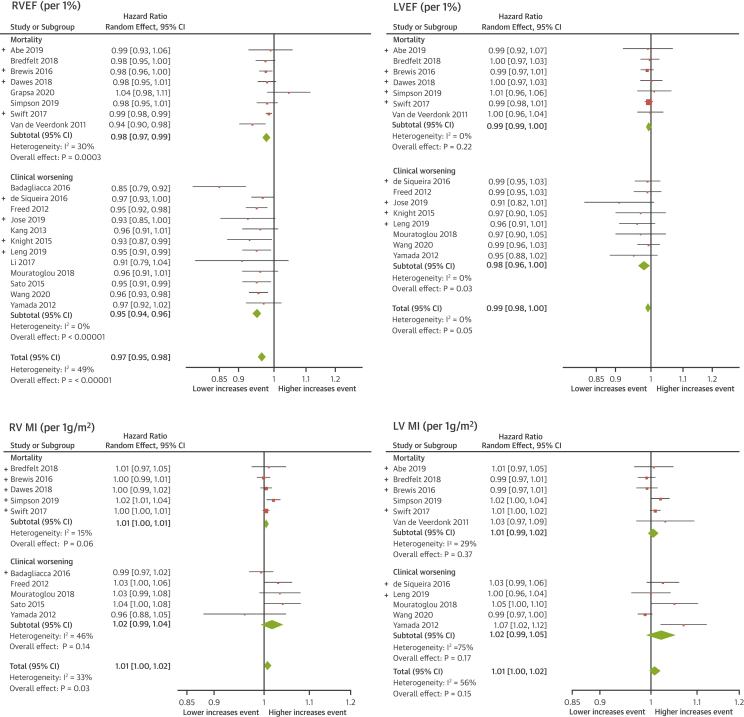
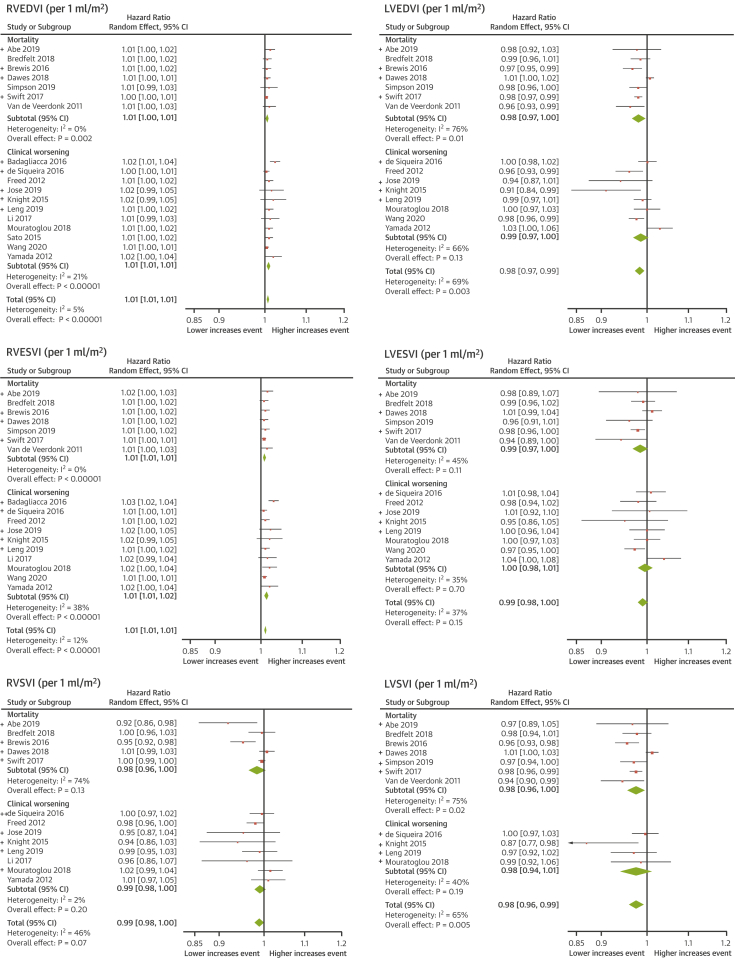
Methods: The Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, and Web of Science databases were searched in May 2020. All CMR studies assessing clinical worsening and the prognosis of patients with PAH were included. Pooled hazard ratios of univariate regression analyses for CMR measurements, for prediction of clinical worsening and mortality, were calculated.
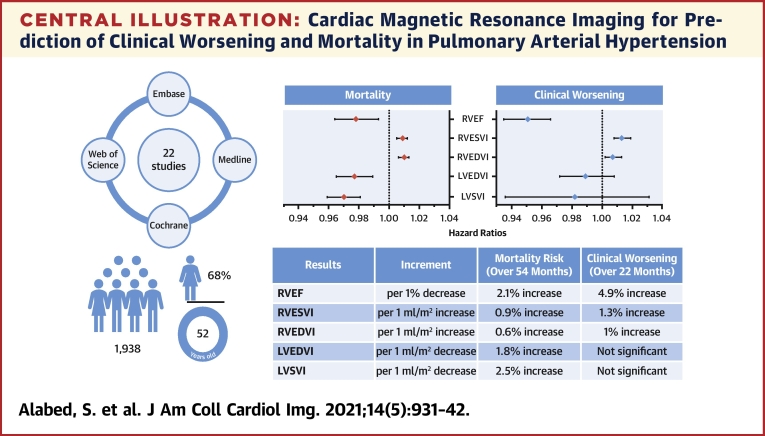
Results: Twenty-two studies with 1,938 participants were included in the meta-analysis. There were 18 clinical worsening events and 8 deaths per 100 patient-years. The pooled hazard ratios show that every 1% decrease in right ventricular (RV) ejection fraction is associated with a 4.9% increase in the risk of clinical worsening over 22 months of follow-up and a 2.1% increase in the risk of death over 54 months. For every 1 ml/m2 increase in RV end-systolic volume index or RV end-diastolic volume index, the risk of clinical worsening increases by 1.3% and 1%, respectively, and the risk of mortality increases by 0.9% and 0.6%. Every 1 ml/m2 decrease in left ventricular stroke volume index or left ventricular end-diastolic volume index increased the risk of death by 2.5% and 1.8%. Left ventricular parameters were not associated with clinical worsening.
Conclusions: This review confirms CMR as a powerful prognostic marker in PAH in a large cohort of patients. In addition to confirming previous observations that RV function and RV and left ventricular volumes predict mortality, RV function and volumes also predict clinical worsening. This study provides a strong rationale for considering CMR as a clinically relevant endpoint for trials of PAH therapies.
Keywords: CMR; PAH; cardiac MRI; meta-analysis; mortality; prognosis; pulmonary arterial hypertension; systematic review.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The study was supported by the Wellcome Trust grants 215799/Z/19/Z and 205188/Z/16/Z. The funder did not have any role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, and approval of the paper. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Cardiac Magnetic Resonance Evaluation of Pulmonary Arterial Hypertension: Transforming From Supplementary to Primary Imaging Modality?JACC Cardiovasc Imaging. 2021 May;14(5):943-946. doi: 10.1016/j.jcmg.2020.11.022. Epub 2021 Jan 13. JACC Cardiovasc Imaging. 2021. PMID: 33454268 Free PMC article. No abstract available.
References
-
- Kiely D.G., Elliot C.A., Sabroe I., Condliffe R. Pulmonary hypertension: diagnosis and management. BMJ. 2013;346:f2028. - PubMed
-
- Galiè N., Humbert M., Vachiery J.L. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2015;46:903–975. - PubMed
-
- McGoon M.D., Benza R.L., Escribano-Subias P. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(Suppl 25):D51–D59. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
