

Regulatory T cell control of systemic immunity and immunotherapy response in liver metastasis
- PMID: 33008914
- PMCID: PMC7755924
- DOI: 10.1126/sciimmunol.aba0759
Regulatory T cell control of systemic immunity and immunotherapy response in liver metastasis
Abstract
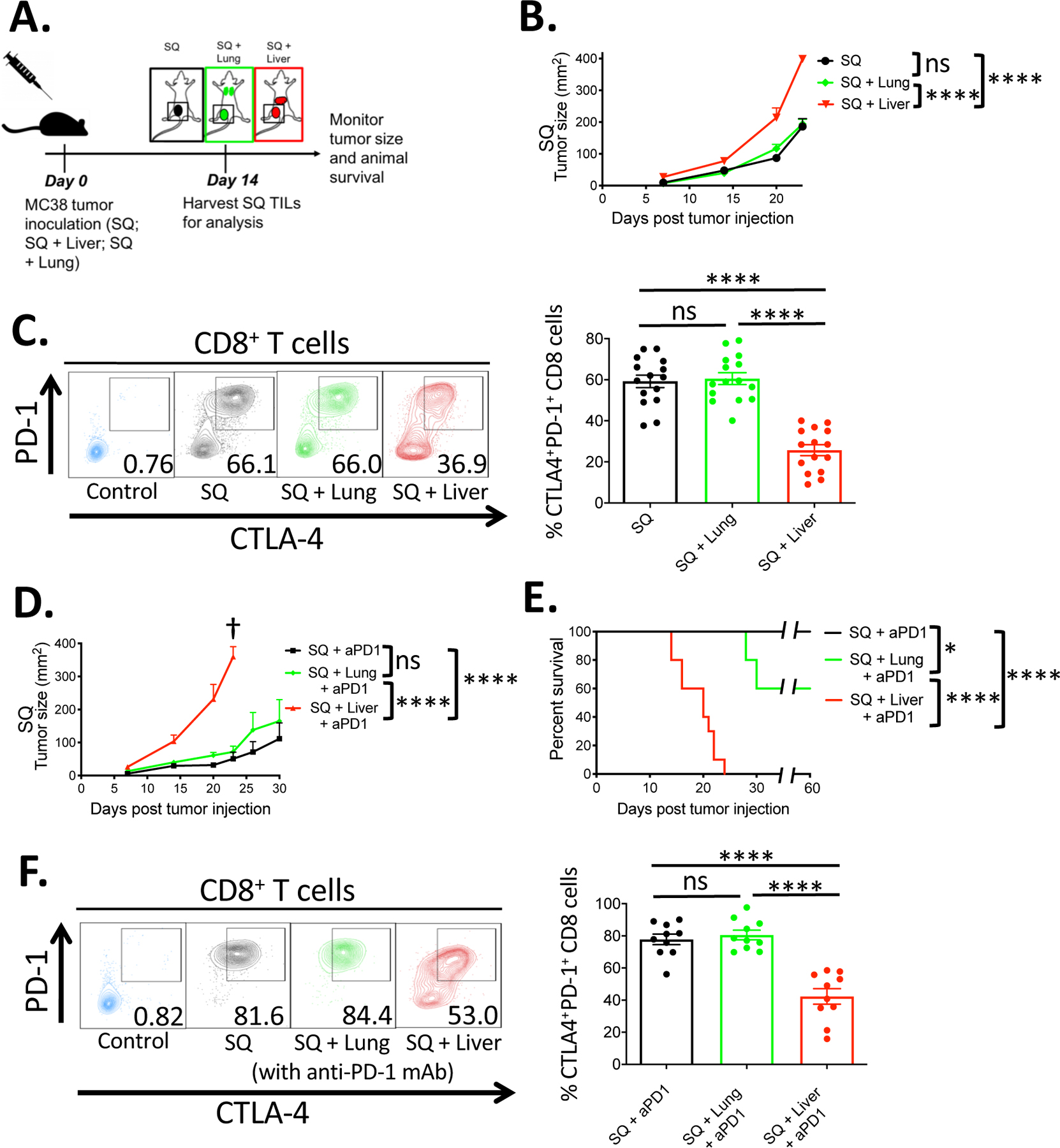
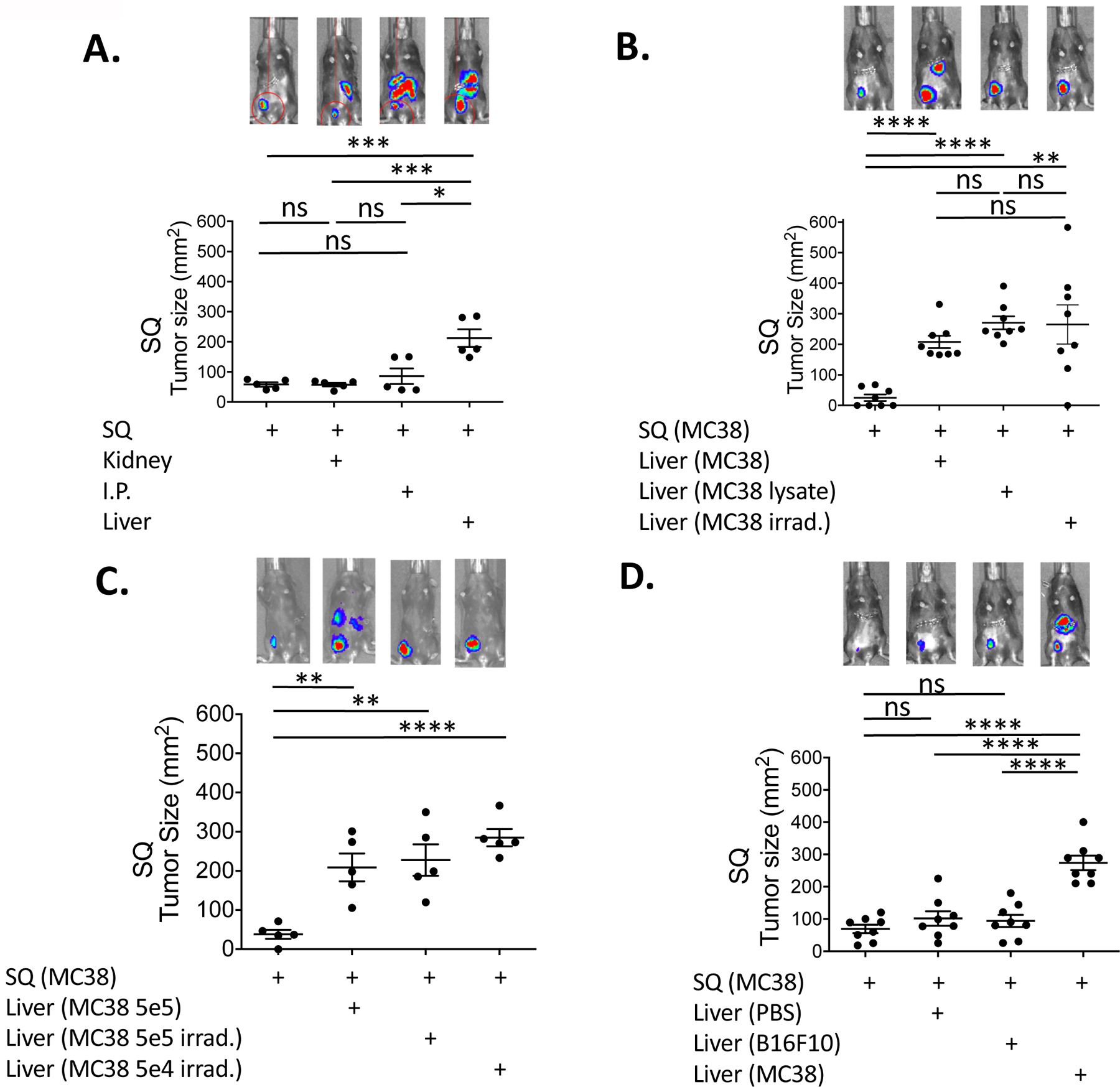
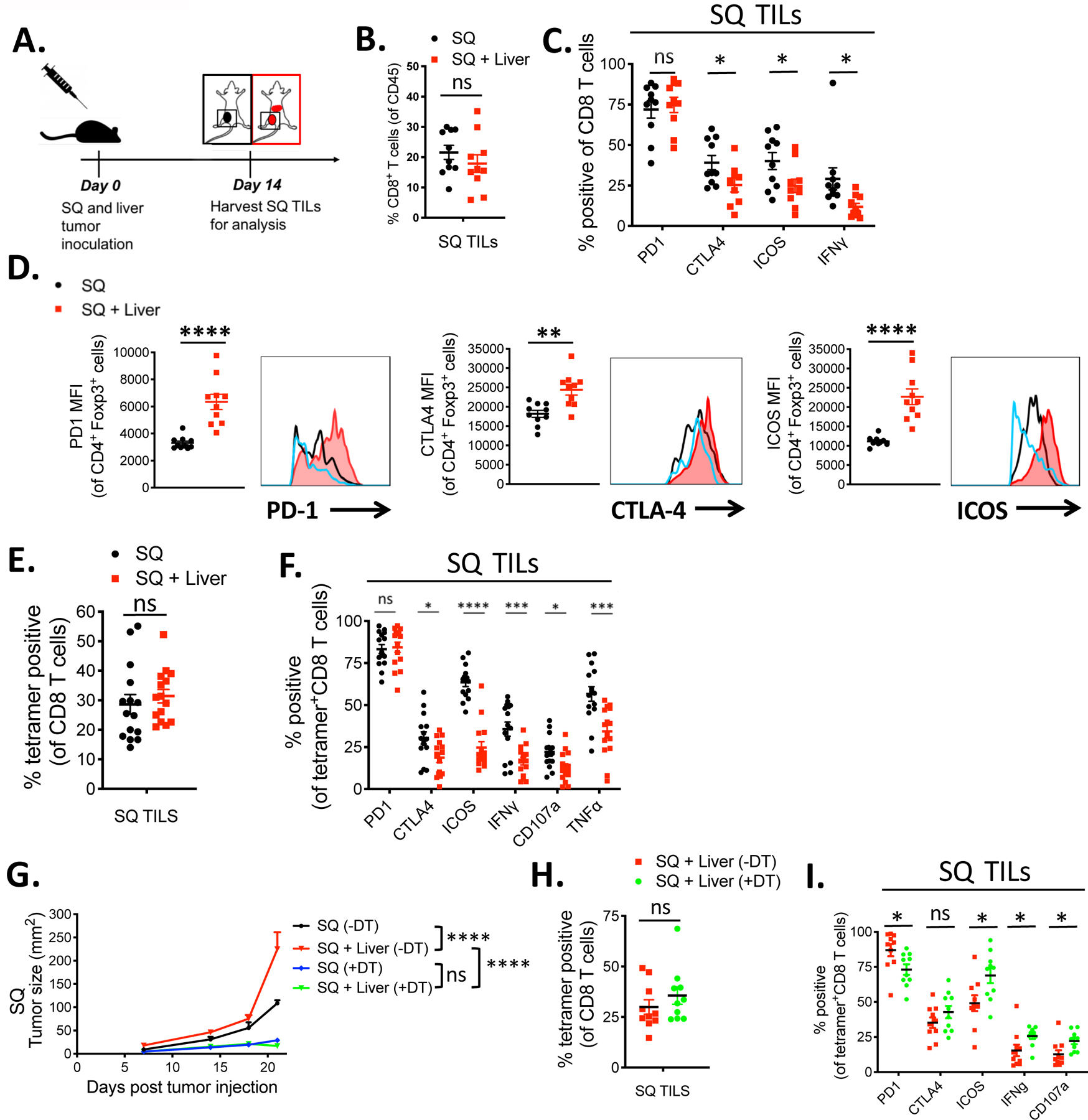
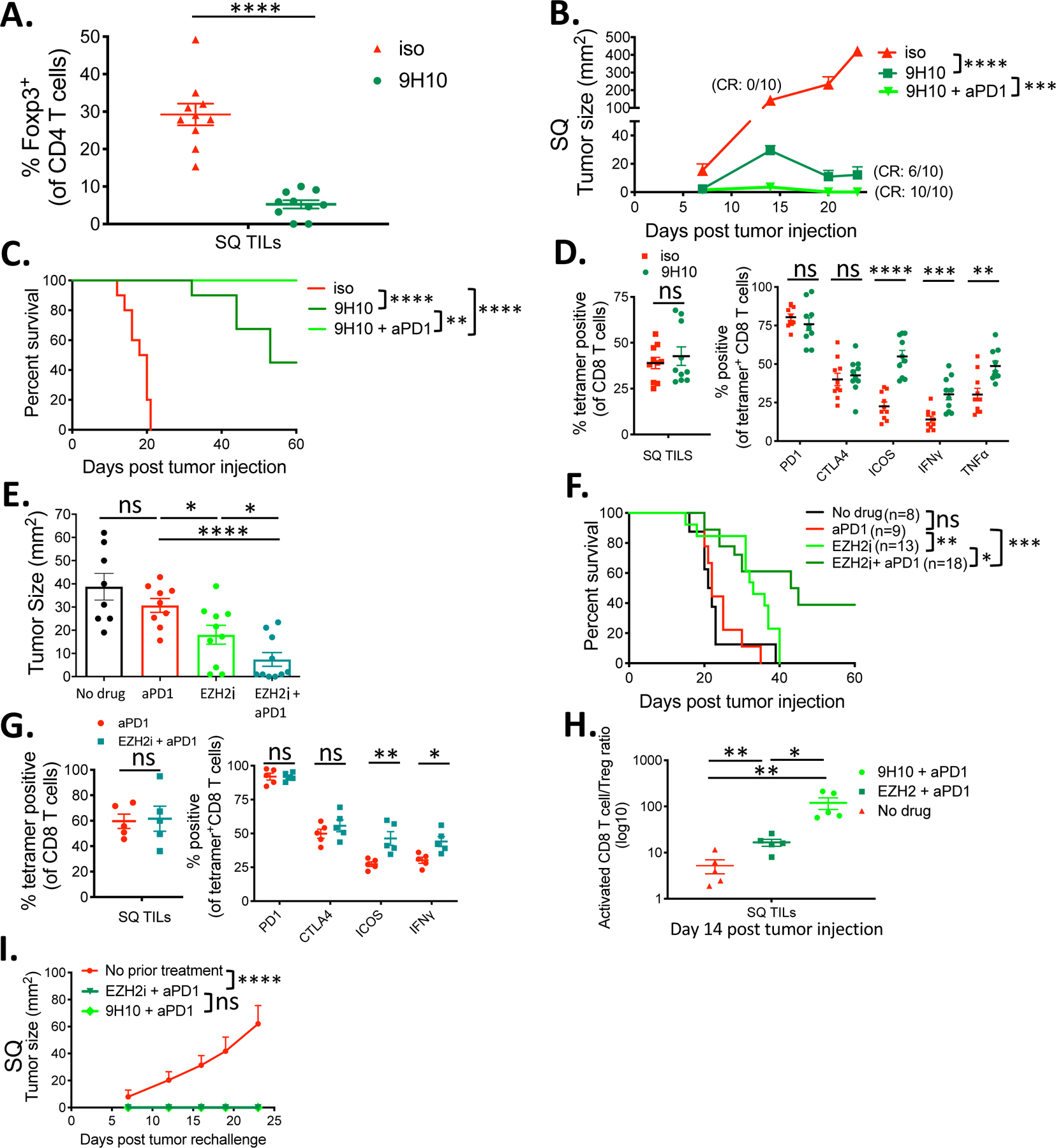
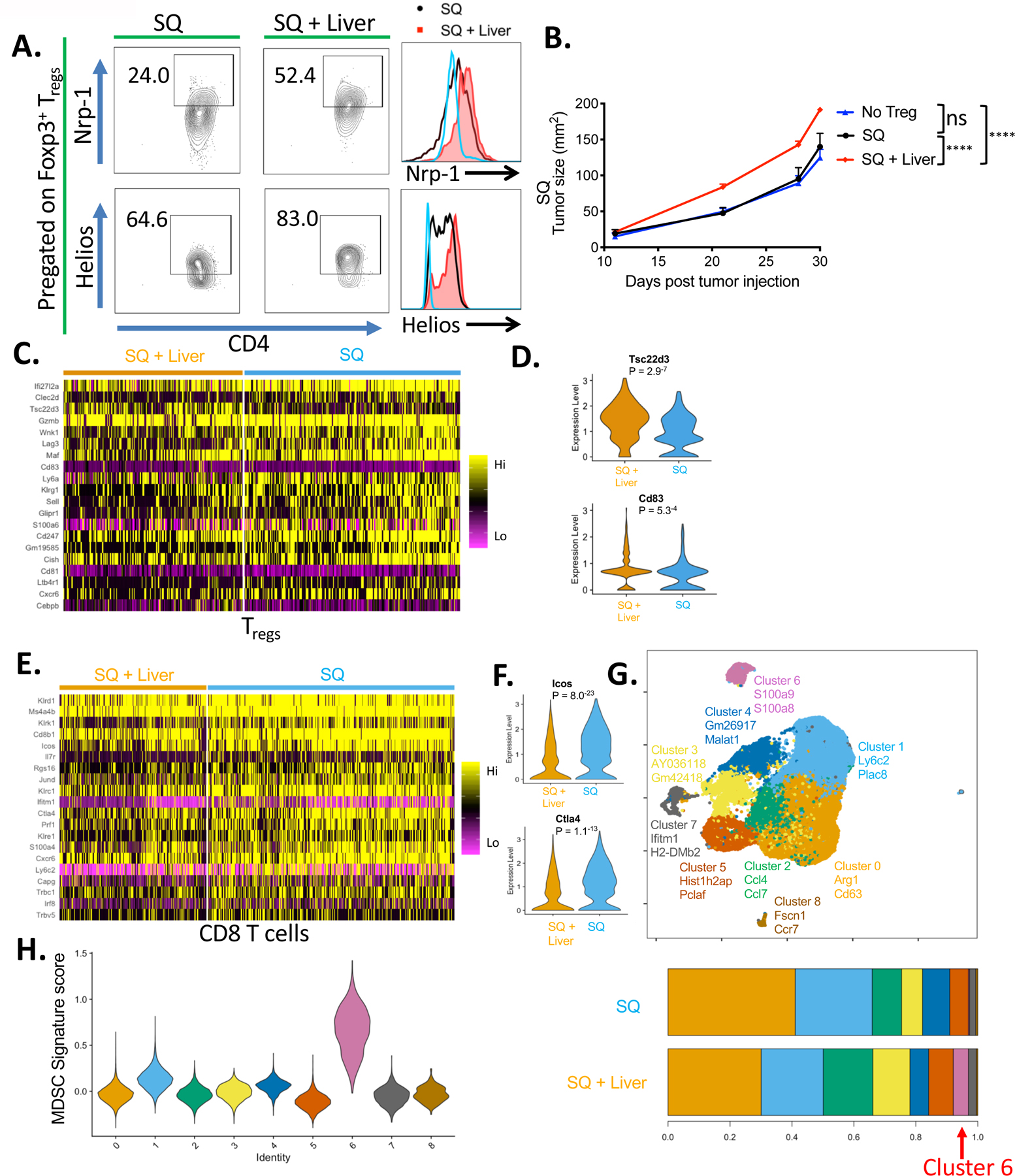
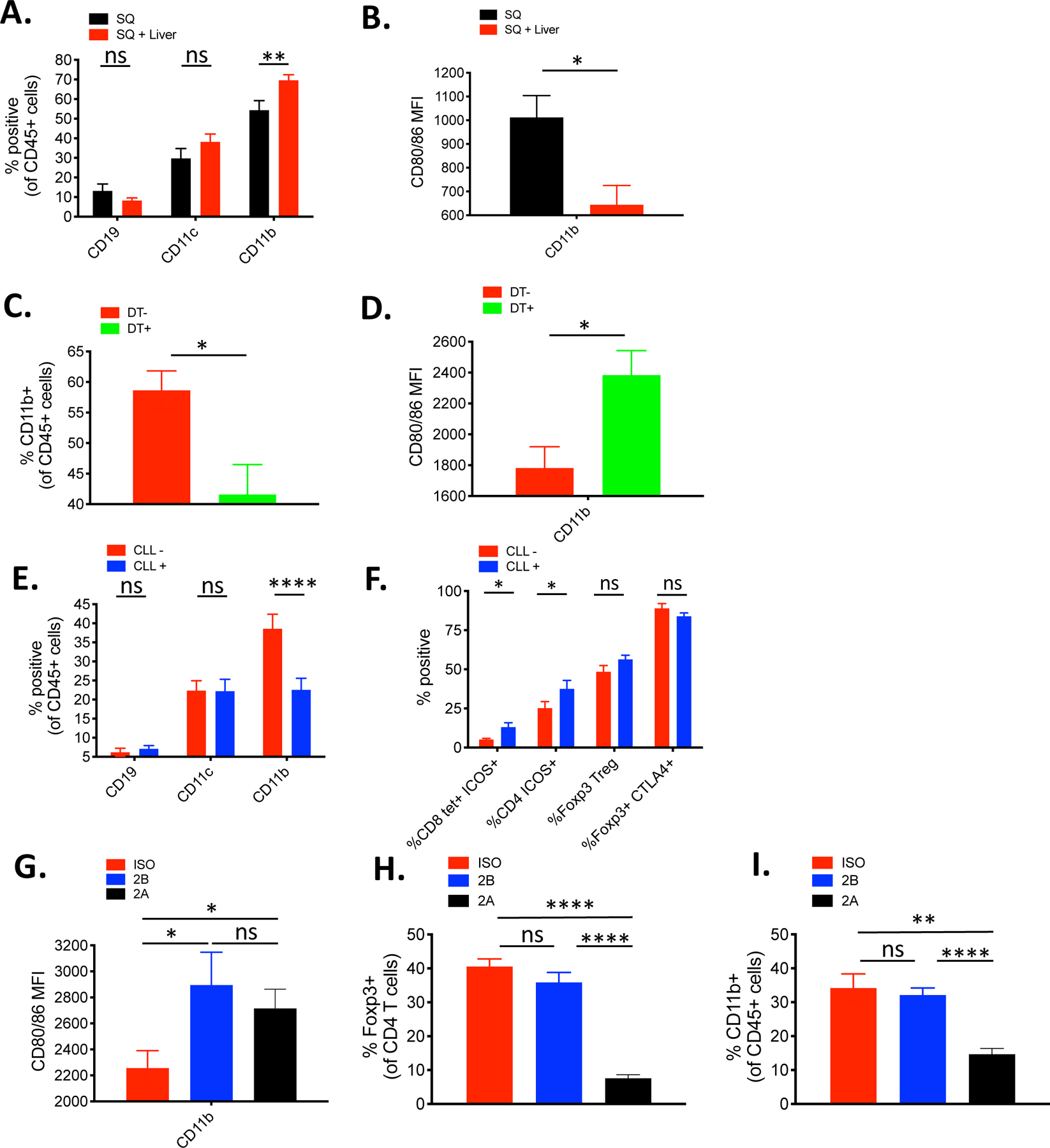
Patients with cancer with liver metastasis demonstrate significantly worse outcomes than those without liver metastasis when treated with anti-PD-1 immunotherapy. The mechanism of liver metastases-induced reduction in systemic antitumor immunity is unclear. Using a dual-tumor immunocompetent mouse model, we found that the immune response to tumor antigen presence within the liver led to the systemic suppression of antitumor immunity. The immune suppression was antigen specific and associated with the coordinated activation of regulatory T cells (Tregs) and modulation of intratumoral CD11b+ monocytes. The dysfunctional immune state could not be reversed by anti-PD-1 monotherapy unless Treg cells were depleted (anti-CTLA-4) or destabilized (EZH2 inhibitor). Thus, this study provides a mechanistic understanding and rationale for adding Treg and CD11b+ monocyte targeting agents in combination with anti-PD-1 to treat patients with cancer with liver metastasis.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
References
-
- Tumeh PC, Hellmann MD, Hamid O, Tsai KK, Loo KL, Gubens MA, Rosenblum M, Harview CL, Taube JM, Handley N, Khurana N, Nosrati A, Krummel MF, Tucker A, Sosa EV, Sanchez PJ, Banayan N, Osorio JC, Nguyen-Kim DL, Chang J, Shintaku IP, Boasberg PD, Taylor EJ, Munster PN, Algazi AP, Chmielowski B, Dummer R, Grogan TR, Elashoff D, Hwang J, Goldinger SM, Garon EB, Pierce RH, Daud A, Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC, Cancer Immunol. Res 5, 417–424 (2017). - PMC - PubMed
-
- Bilen MA, Shabto JM, Martini DJ, Liu Y, Lewis C, Collins HH, Akce M, Kissick H, Carthon BC, Shaib WL, Alese OB, Steuer CE, Wu C, Lawson DH, Kudchadkar R, Master V, El-Rayes B, Ramalingam SS, Owonikoko TK, Harvey RD, Sites of metastasis and association with clinical outcome (CO) in advanced stage cancer patients (pts) treated with immunotherapy (IO), BMC Cancer 19 (2019), 10.1093/annonc/mdy288.092. - DOI - PMC - PubMed
-
- Sasaki A, Nakamura Y, Mishima S, Kawazoe A, Kuboki Y, Bando H, Kojima T, Doi T, Ohtsu A, Yoshino T, Kuwata T, Akimoto T, Shitara K, Predictive factors for hyperprogressive disease during nivolumab as anti-PD1 treatment in patients with advanced gastric cancer, Gastric Cancer (2019), 10.1007/s10120-018-00922-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
