

Evaluation of Automated Video Monitoring to Decrease the Risk of Unattended Bed Exits in Small Rural Hospitals
- PMID: 33009181
- PMCID: PMC8612902
- DOI: 10.1097/PTS.0000000000000789
Evaluation of Automated Video Monitoring to Decrease the Risk of Unattended Bed Exits in Small Rural Hospitals
Abstract
Objectives: This study aimed to evaluate the effectiveness of using 1 to 4 mobile or fixed automated video monitoring systems (AVMSs) to decrease the risk of unattended bed exits (UBEs) as antecedents to unassisted falls among patients at high risk for falls and fall-related injuries in 15 small rural hospitals.
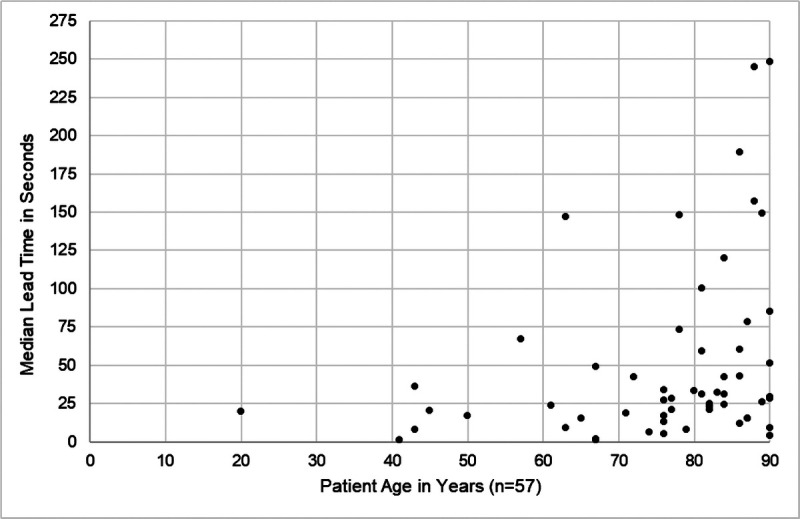
Methods: We compared UBE rates and fall rates during baseline (5 months in which patient movement was recorded but nurses did not receive alerts) and intervention phases (2 months in which nurses received alerts). We determined lead time (seconds elapsed from the first alert because of patient movement until 3 seconds after an UBE) during baseline and positive predictive value and sensitivity during intervention.
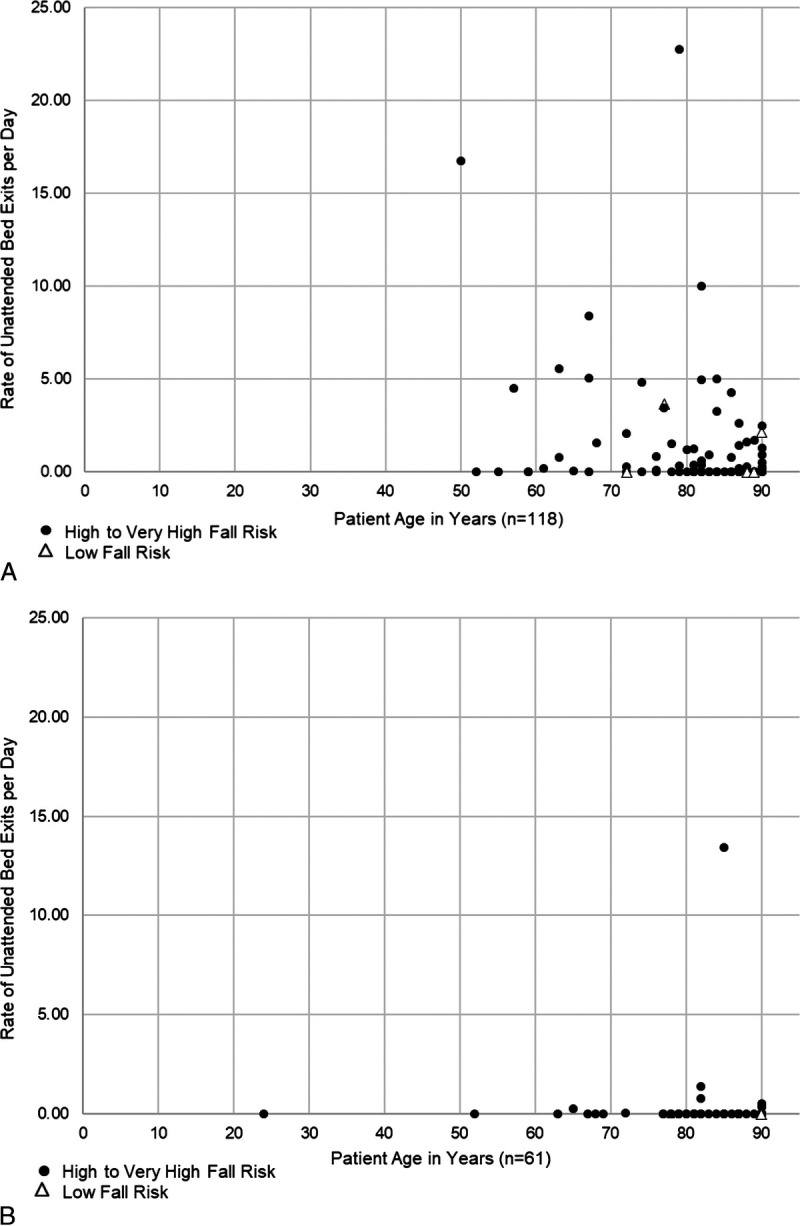
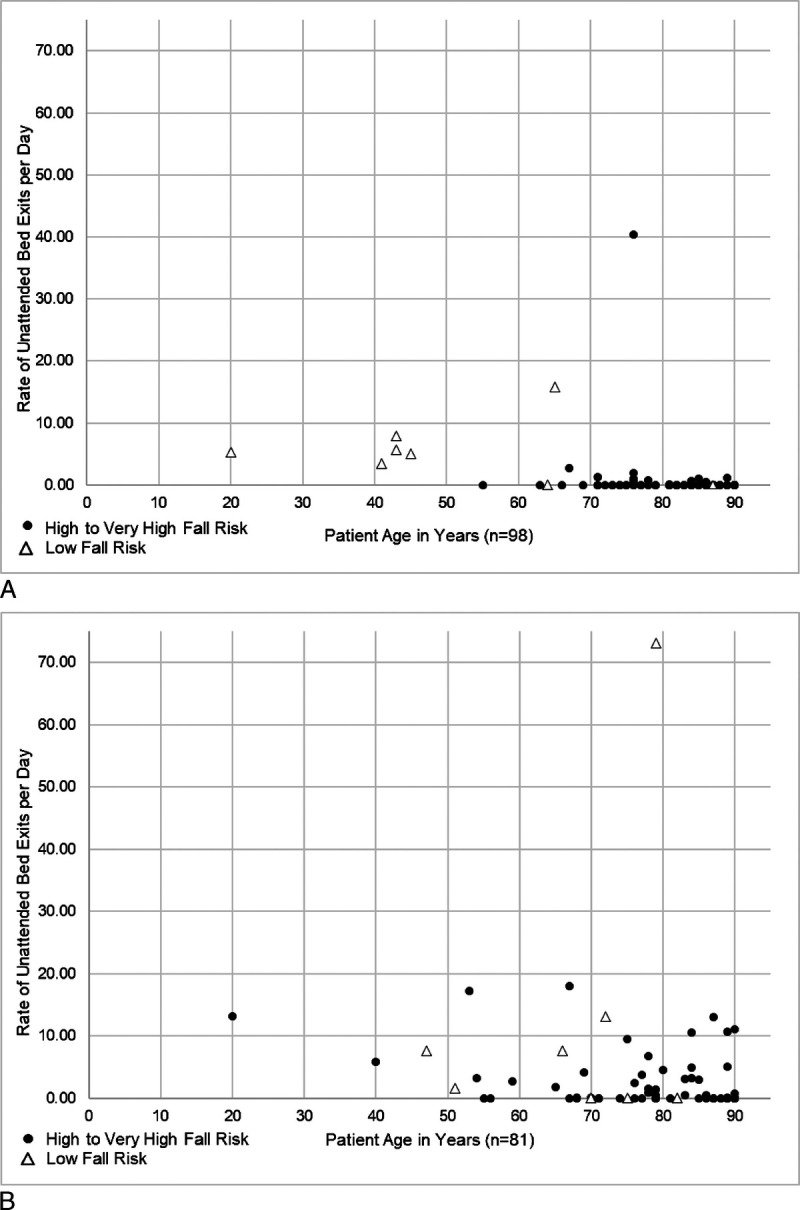
Results: Age and fall risk were negatively associated with the baseline patient rate of UBEs/day. From baseline to intervention: in 9 hospitals primarily using mobile systems, UBEs/day decreased from 0.84 to 0.09 (89%); in 5 hospitals primarily using fixed systems, UBEs/day increased from 0.43 to 3.18 (649%) as patients at low risk for falls were observed safely exiting the bed; and among 13 hospitals with complete data, total falls/1000 admissions decreased from 8.83 to 5.53 (37%), and injurious falls/1000 admissions decreased from 2.52 to 0.55 (78%). The median lead time of the AVMS was 28.5 seconds, positive predictive value was nearly 60%, and sensitivity was 97.4%.
Conclusions: Use of relatively few AVMSs may allow nurses to adaptively manage UBEs as antecedents to unassisted falls and fall-related injuries in small rural hospitals. Additional research is needed in larger hospitals to better understand the effectiveness of AVMSs.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
K.J. was an associate professor in the College of Allied Health Professions at the University of Nebraska Medical Center until June 2018, when she retired. She completed this article as an independent contractor. L.S. is employed by Ocuvera, LLC, and has an ownership interest in the company; he did not participate in data analysis. G.H. has no conflicts of interest to declare.
Figures


References
-
- Oliver D, Healey F, Haines TP. Preventing falls and fall-related injuries in hospitals. Clin Geriatr Med. 2010;26:645–692. - PubMed
-
- Weiss AJ, Elixhauser A, eds. Overview of Hospital Stays in the United States, 2012. Rockville, MD: Agency for Healthcare Research and Quality; October 2014 HCUP Statistical Brief; No. 180. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-Un.... Accessed February 26, 2020. - PubMed
-
- Morello RT Barker AL Watts JJ, et al. The extra resource burden of in-hospital falls: a cost of falls study. Med J Aust. 2015;203:367. - PubMed
-
- Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med. 2002;18:141–158. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
