

How Satisfied Are Patients and Surgeons with Telemedicine in Orthopaedic Care During the COVID-19 Pandemic? A Systematic Review and Meta-analysis
- PMID: 33009231
- PMCID: PMC7899486
- DOI: 10.1097/CORR.0000000000001494
How Satisfied Are Patients and Surgeons with Telemedicine in Orthopaedic Care During the COVID-19 Pandemic? A Systematic Review and Meta-analysis
Abstract
Background: The coronavirus disease 2019 pandemic has resulted in a rapid pivot toward telemedicine owing to closure of in-person elective clinics and sustained efforts at physical distancing worldwide. Throughout this period, there has been revived enthusiasm for delivering and receiving orthopaedic care remotely. Unfortunately, rapidly published editorials and commentaries during the pandemic have not adequately conveyed findings of published randomized trials on this topic.
Questions/purposes: In this systematic review and meta-analysis of randomized trials, we asked: (1) What are the levels of patient and surgeon satisfaction with the use of telemedicine as a tool for orthopaedic care delivery? (2) Are there differences in patient-reported outcomes between telemedicine visits and in-person visits? (3) What is the difference in time commitment between telemedicine and in-person visits?
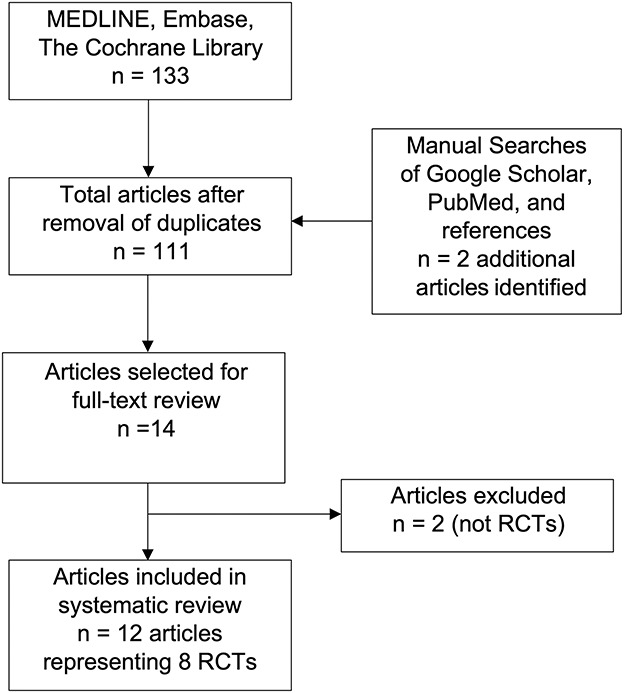
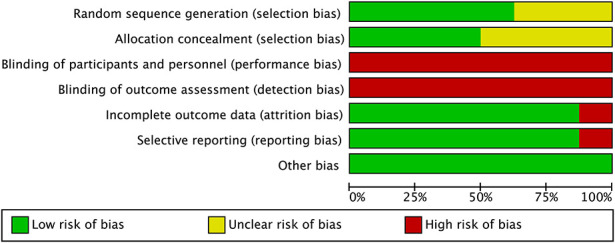
Methods: In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we conducted a systematic review with the primary objective to determine patient and surgeon satisfaction with telemedicine, and secondary objectives to determine differences in patient-reported outcomes and time commitment. We used combinations of search keywords and medical subject headings around the terms "telemedicine", "telehealth", and "virtual care" combined with "orthopaedic", "orthopaedic surgery" and "randomized." We searched three medical databases (MEDLINE, Embase, and the Cochrane Library) in duplicate and performed manual searches to identify randomized controlled trials evaluating the outcomes of telemedicine and in-person orthopaedic assessments. Trials that studied an intervention that was considered to be telemedicine (that is, any form of remote or virtual care including, but not limited to, video, telephone, or internet-based care), had a control group that comprised in-person assessments performed by orthopaedic surgeons, and were reports of Level I original evidence were included in this study. Studies evaluating physiotherapy or rehabilitation interventions were excluded. Data was extracted by two reviewers and quantitative and qualitive summaries of results were generated. Methodological quality of included trials was assessed using the Cochrane Risk of Bias tool, which uniformly rated the trials at high risk of bias within the blinding categories (blinding of providers, patients, and outcome assessors). We screened 133 published articles; 12 articles (representing eight randomized controlled trials) met the inclusion criteria. There were 1008 patients randomized (511 to telemedicine groups and 497 to control groups). Subspecialties represented were hip and knee arthroplasty (two trials), upper extremity (two trials), pediatric trauma (one trial), adult trauma (one trial), and general orthopaedics (two trials).
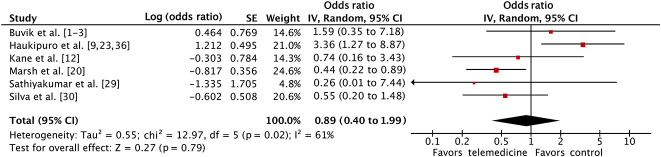
Results: There was no difference in the odds of satisfaction between patients receiving telemedicine care and those receiving in-person care (pooled odds ratio 0.89 [95% CI 0.40 to 1.99]; p = 0.79). There were also no differences in surgeon satisfaction (pooled OR 0.38 [95% CI 0.07 to 2.19]; p = 0.28) or among multiple patient-reported outcome measures that evaluated pain and function. Patients reported time savings, both when travel time was excluded (17 minutes shorter [95% CI 2 to 32]; p = 0.03) and when it was included (180 minutes shorter [95% CI 78 to 281]; p < 0.001).
Conclusion: Evidence from heterogeneous randomized studies demonstrates that the use of telemedicine for orthopaedic assessments does not result in identifiable differences in patient or surgeon satisfaction compared with in-person assessments. Importantly, the source studies in this review did not adequately capture or report safety endpoints, such as complications or missed diagnoses. Future studies must be adequately powered to detect these differences to ensure patient safety is not compromised with the use of telemedicine. Although telemedicine may lead to a similar patient experience, surgeons should maintain a low threshold for follow-up with in-person assessments whenever possible in the absence of further safety data.
Level of evidence: Level I, therapeutic study.
Copyright © 2020 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that he, nor any member of his immediate family, has funding or commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: How Satisfied Are Patients and Surgeons with Telemedicine in Orthopaedic Care During the COVID-19 Pandemic? A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2021 Jan 1;479(1):57-59. doi: 10.1097/CORR.0000000000001594. Clin Orthop Relat Res. 2021. PMID: 33315621 Free PMC article. No abstract available.
References
-
- Buvik A, Bugge E, Knutsen G, Smabrekke A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25:451-459. - PubMed
-
- Delaigue S, Bonnardot L, Steichen O, Garcia DM, Venugopal R, Saint-Sauveur JF, Wootton R. Seven years of telemedicine in Medecins Sans Frontieres demonstrate that offering direct specialist expertise in the frontline brings clinical and educational value. J Glob Health. 2018;8:020414. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
