

Early Antibiotic Administration Is Associated with a Reduced Infection Risk When Combined with Primary Wound Closure in Patients with Open Tibia Fractures
- PMID: 33009232
- PMCID: PMC7899592
- DOI: 10.1097/CORR.0000000000001507
Early Antibiotic Administration Is Associated with a Reduced Infection Risk When Combined with Primary Wound Closure in Patients with Open Tibia Fractures
Erratum in
-
Erratum to: Early Antibiotic Administration Is Associated With a Reduced Infection Risk When Combined With Primary Wound Closure in Patients With Open Tibia Fractures.Clin Orthop Relat Res. 2023 Mar 1;481(3):627. doi: 10.1097/CORR.0000000000002583. Epub 2023 Feb 8. Clin Orthop Relat Res. 2023. PMID: 36752764 Free PMC article. No abstract available.
Abstract
Background: Early administration of antibiotics and wound coverage have been shown to decrease the deep infection risk in all patients with Type 3 open tibia fractures. However, it is unknown whether early antibiotic administration decreases infection risk in patients with Types 1, 2, and 3A open tibia fractures treated with primary wound closure.
Questions/purposes: (1) Does decreased time to administration of the first dose of antibiotics decrease the deep infection risk in all open tibia fractures with primary wound closure? (2) What patient demographic factors are associated with an increased deep infection risk in Types 1, 2, and 3A open tibia fractures with primary wound closure?
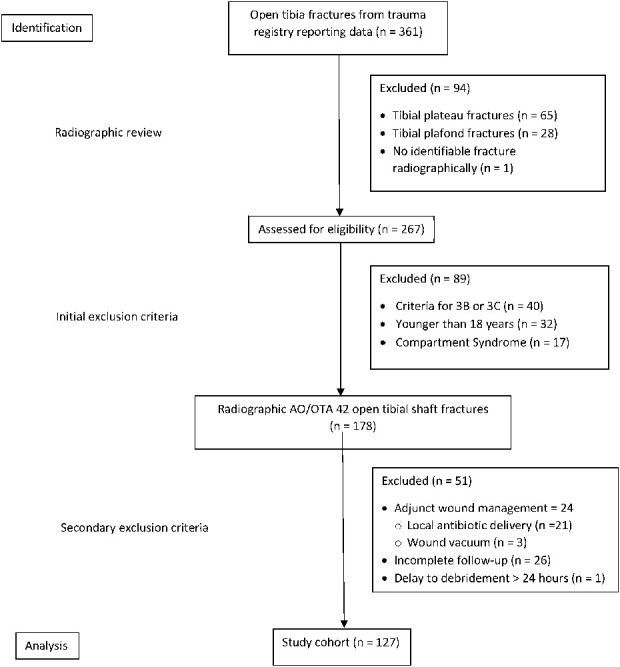
Methods: We identified 361 open tibia fractures over a 5-year period at a Level I regional trauma center that receives direct admissions and transfers from other hospitals which produces large variation in the timing of antibiotic administration. Patients were excluded if they were younger than 18 years, had associated plafond or plateau fractures, associated with compartment syndrome, had a delay of more than 24 hours from injury to the operating room, underwent repeat débridement procedures, had incomplete data, and were treated with negative-pressure dressings or other adjunct wound management strategies that would preclude primary closure. Primary closure was at the descretion of the treating surgeon. We included patients with a minimum follow-up of 6 weeks with assessment at 6 months and 12 months. One hundred forty-three patients with were included in the analysis. Our primary endpoint was deep infection as defined by the CDC criteria. We obtained chronological data, including the time to the first dose of antibiotics and time to surgical débridement from ambulance run sheets, transferring hospital records, and the electronic medical record to answer our first question. We considered demographics, American Society of Anesthesiologists classification, mechanism of injury, smoking status, presence of diabetes, and Injury Severity Score in our analysis of other factors. These were compared using one-way ANOVA, chi-square, or Fisher's exact tests. Binary regression was used to to ascertain whether any factors were associated with postoperative infection. Receiver operator characteristic curves were used to identify threshold values.
Results: Increased time to first administration of antibiotics was associated with an increased infection risk in patients who were treated with primary wound closure; the greatest inflection point on that analysis occurred at 150 minutes, when the increased infection risk was greatest (20% [8 of 41] versus 4% [3 of 86]; odds ratio 5.6 [95% CI 1.4 to 22.2]; p = 0.01). After controlling for potential confounding variables like age, diabetes and smoking status, none of the variables we evaluated were associated with an increased risk of deep infection in Type 1, 2, and 3A open tibia fractures in patients treated with primary wound closure.
Conclusion: Our findings suggest that in open tibia fractures, which receive timely antibiotic administration, primary wound closure is associated with a decreased infection risk. We recognize that more definitive studies need to be performed to confirm these findings and confirm feasibility of early antibiotic administration, especially in the pre-hospital context.
Level of evidence: Level III, therapeutic study.
Copyright © 2020 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that he has no commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Early Antibiotic Administration Is Associated with a Reduced Infection Risk When Combined with Primary Wound Closure in Patients.Clin Orthop Relat Res. 2021 Mar 1;479(3):620-622. doi: 10.1097/CORR.0000000000001545. Clin Orthop Relat Res. 2021. PMID: 33079772 Free PMC article. No abstract available.
References
-
- Al-Arabi YB, Nader M, Hamidian-Jahromi AR, Woods DA. The effect of the timing of antibiotics and surgical treatment on infection rates in open long-bone fractures: a 9-year prospective study from a district general hospital [published correction appears in Injury. 2008;39:381 Nader, Michael [corrected to Nader, Maher]. Injury. 2007;38:900-905. - PubMed
-
- Baker SP, O’Neill B, Haddon W, Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187-196. - PubMed
-
- Benson DR, Riggins RS, Lawrence RM, Hoeprich PD, Huston AC, Harrison JA. Treatment of open fractures: a prospective study. J Trauma. 1983;23:25-30. - PubMed
-
- Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, Sanders RW, Jones AL, McAndrew MP, Patterson BM, McCarthy ML, Travison TG, Castillo RC. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med . 2002;347:1924-1931. - PubMed
-
- Butler F, O’Connor K. Antibiotics in tactical combat casualty care 2002. Mil Med. 2003;168:911-914. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
