

Real-world data from a molecular tumor board demonstrates improved outcomes with a precision N-of-One strategy
- PMID: 33009371
- PMCID: PMC7532150
- DOI: 10.1038/s41467-020-18613-3
Real-world data from a molecular tumor board demonstrates improved outcomes with a precision N-of-One strategy
Abstract
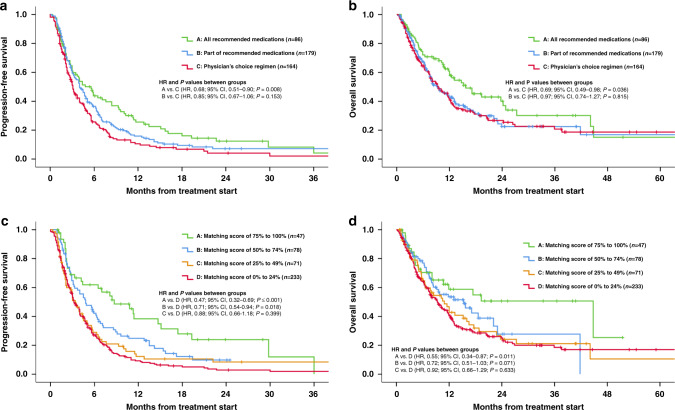
Next-generation sequencing (NGS) can identify novel cancer targets. However, interpreting the molecular findings and accessing drugs/clinical trials is challenging. Furthermore, many tumors show resistance to monotherapies. To implement a precision strategy, we initiated a multidisciplinary (basic/translational/clinical investigators, bioinformaticians, geneticists, and physicians from multiple specialties) molecular tumor board (MTB), which included a project manager to facilitate obtaining clinical-grade biomarkers (blood/tissue NGS, specific immunohistochemistry/RNA expression including for immune-biomarkers, per physician discretion) and medication-acquisition specialists/clinical trial coordinators/navigators to assist with medication access. The MTB comprehensively reviewed patient characteristics to develop N-of-One treatments implemented by the treating physician's direction under the auspices of a master protocol. Overall, 265/429 therapy-evaluable patients (62%) were matched to ≥1 recommended drug. Eighty-six patients (20%) matched to all drugs recommended by MTB, including combinatorial approaches, while 38% received physician's choice regimen, generally with unmatched approach/low degree of matching. Our results show that patients who receive MTB-recommended regimens (versus physician choice) have significantly longer progression-free (PFS) and overall survival (OS), and are better matched to therapy. High (≥50%) versus low (<50%) Matching Score therapy (roughly reflecting therapy matched to ≥50% versus <50% of alterations) independently correlates with longer PFS (hazard ratio [HR], 0.63; 95% confidence interval [CI], 0.50-0.80; P < 0.001) and OS (HR, 0.67; 95% CI, 0.50-0.90; P = 0.007) and higher stable disease ≥6 months/partial/complete remission rate (52.1% versus 30.4% P < 0.001) (all multivariate). In conclusion, patients who receive MTB-based therapy are better matched to their genomic alterations, and the degree of matching is an independent predictor of improved oncologic outcomes including survival.
Conflict of interest statement
S.K. serves as a consultant for Foundation Medicine and receives speaker’s fees from Roche. R.E. serves as a consultant for GSK, Merck, Eisai, Clovis Oncology, AstraZenica, Pfizer and Iovance. He has received speaker fees from AstraZenica and Merck. A.S. reports research funding and honoraria from Pfizer and Varian Medical Systems, consultant fees from AstraZeneca and Jounce Therapeutics, personal fees from Merck, and is the scientific founder with equity interest in Toragen Inc. outside the submitted work. J.K.S. receives research funds from Foundation Medicine Inc. and Amgen, as well as consultant fees from Grand Rounds, Deciphera and LOXO. R.K. has research funding from Incyte, Genentech, Merck Serono, Pfizer, Sequenom, Foundation Medicine, Guardant Health, Grifols, and Konica Minolta, as well as consultant fees from LOXO, X-Biotech, Actuate Therapeutics, Genentec, Pfizer and NeoMed. She receives speaker fees from Roche, and has an equity interest in IDbyDNA and Curematch, Inc. She is a co-founder of CureMatch and Board member of CureMatch and CureMetrix. The remaining authors declare no competing interests.
Figures


References
-
- Drilon A, et al. Safety and antitumor activity of the multitargeted pan-TRK, ROS1, and ALK inhibitor entrectinib: combined results from two phase I trials (ALKA-372-001 and STARTRK-1) Cancer Disco. 2017;7:400–409. doi: 10.1158/2159-8290.CD-16-1237. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
