

Increased pulmonary serotonin transporter in patients with chronic obstructive pulmonary disease who developed pulmonary hypertension
- PMID: 33009594
- PMCID: PMC8041706
- DOI: 10.1007/s00259-020-05056-7
Increased pulmonary serotonin transporter in patients with chronic obstructive pulmonary disease who developed pulmonary hypertension
Abstract
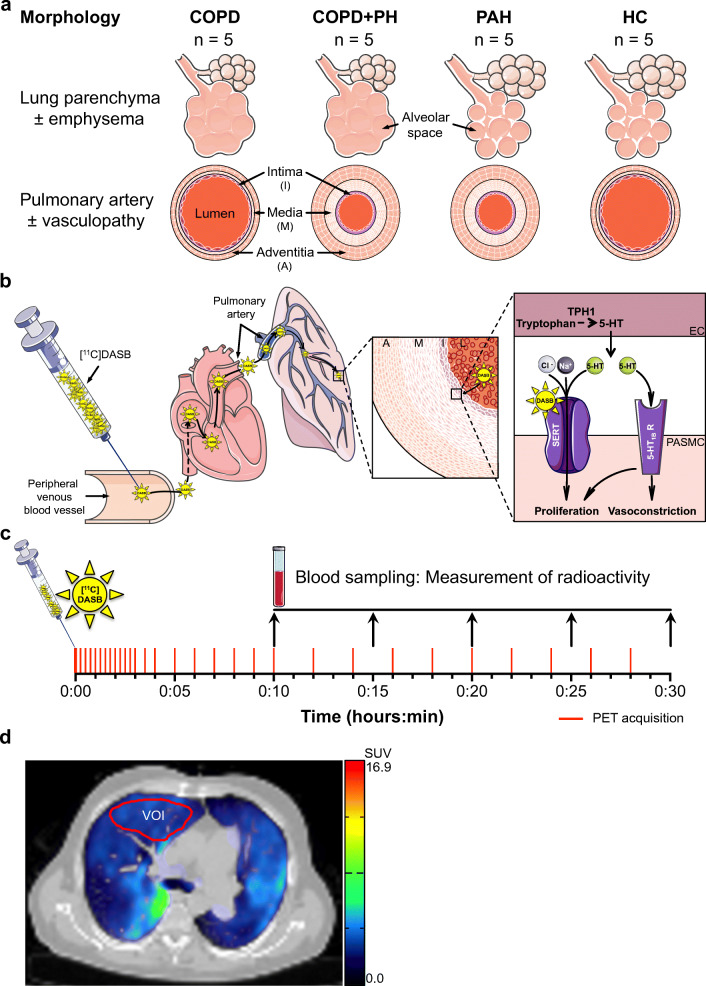
Purpose: Pulmonary hypertension (PH) is characterized by a progressive remodelling of the pulmonary vasculature resulting in right heart failure and eventually death. The serotonin transporter (SERT) may be involved in the pathogenesis of PH in patients with chronic-obstructive pulmonary disease (COPD). This study investigated for the first time the SERT in vivo availability in the lungs of patients with COPD and PH (COPD+PH).
Methods: SERT availability was assessed using SERT-selective [11C]DASB and positron emission tomography/computed tomography (PET/CT) with dynamic acquisition over 30 min in 4 groups of 5 participants each: COPD, COPD+PH, pulmonary arterial hypertension, and a healthy control (HC). Time activity curves were generated based on a volume of interest within the middle lobe. Tissue-to-blood concentration ratios after 25 to 30 min (TTBR25-30) served as receptor parameter for group comparison and were corrected for lung tissue attenuation. Participants underwent comprehensive pulmonary workup. Statistical analysis included group comparisons and correlation analysis.
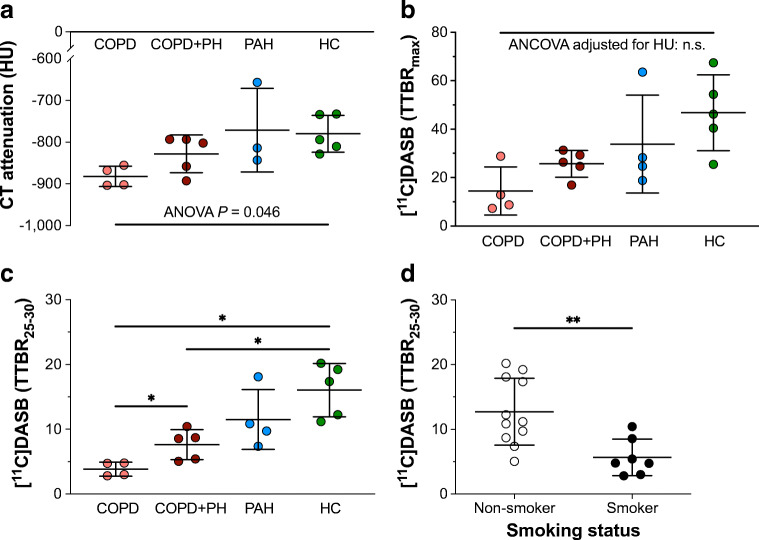
Results: [11C]DASB uptake peak values did not differ among the cohorts after adjusting for lung tissue attenuation, suggesting equal radiotracer delivery. Both the COPD and COPD+PH cohort showed significantly lower TTBR25-30 values after correction for lung attenuation than HC. Attenuation corrected TTBR25-30 values were significantly higher in the COPD+PH cohort than those in the COPD cohort and higher in non-smokers than in smokers. They positively correlated with invasively measured severity of PH and inversely with airflow limitation and emphysema. Considering all COPD patients ± PH, they positively correlated with right heart strain (NT-proBNP).
Conclusion: By applying [11C]DASB and PET/CT, semiquantitative measures of SERT availability are demonstrated in the lung vasculature of patients with COPD and/or PH. COPD patients who developed PH show increased pulmonary [11C]DASB uptake compared to COPD patients without PH indicating an implication of pulmonary SERT in the development of PH in COPD patients.
Keywords: Chronic obstructive pulmonary disease; Computed tomography; Positron emission tomography; Pulmonary hypertension; Serotonin transporter.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Computed tomographic measurement of airway remodeling and emphysema in advanced chronic obstructive pulmonary disease. Correlation with pulmonary hypertension.Am J Respir Crit Care Med. 2015 Jan 1;191(1):63-70. doi: 10.1164/rccm.201408-1423OC. Am J Respir Crit Care Med. 2015. PMID: 25393421
-
Characteristics of Chronic Obstructive Pulmonary Disease Patients with Pulmonary Hypertension Assessed by Echocardiography in a Three-Year Observational Cohort Study.Int J Chron Obstruct Pulmon Dis. 2020 Mar 3;15:487-499. doi: 10.2147/COPD.S230952. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32184586 Free PMC article.
-
Assessing pulmonary hypertension in COPD. Is there a role for computed tomography?Int J Chron Obstruct Pulmon Dis. 2019 Sep 4;14:2065-2079. doi: 10.2147/COPD.S207363. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 31564854 Free PMC article. Review.
-
Quantitative computed tomography of pulmonary emphysema and ventricular function in chronic obstructive pulmonary disease patients with pulmonary hypertension.Korean J Radiol. 2014 Nov-Dec;15(6):871-7. doi: 10.3348/kjr.2014.15.6.871. Epub 2014 Nov 7. Korean J Radiol. 2014. PMID: 25469102 Free PMC article.
-
Pulmonary hypertension in chronic lung diseases.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D109-16. doi: 10.1016/j.jacc.2013.10.036. J Am Coll Cardiol. 2013. PMID: 24355635 Review.
Cited by
-
Expression Patterns of Serotonin Receptors 5-HT1A, 5-HT2A, and 5-HT3A during Human Fetal Lung Development.Int J Mol Sci. 2023 Feb 3;24(3):2965. doi: 10.3390/ijms24032965. Int J Mol Sci. 2023. PMID: 36769290 Free PMC article.
-
The Influence of Serotonergic Signaling on Quality of Life, Depression, Insomnia, and Hypoxia in Obstructive Sleep Apnea Patients: Cross-Sectional Study.J Clin Med. 2025 Jan 12;14(2):445. doi: 10.3390/jcm14020445. J Clin Med. 2025. PMID: 39860451 Free PMC article.
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) Eur Respir J. 2015;46(4):903–975. doi: 10.1183/13993003.01032-2015. - DOI - PubMed
-
- Global initiative for chronic obstructive lung disease. Global strategy for diagnosis, management and prevention of COPD (2020 Report). www.goldcopd.org. 2019. Accessed 16 Nov 2019.
-
- Eddahibi S, Guignabert C, Barlier-Mur AM, Dewachter L, Fadel E, Dartevelle P, et al. Cross talk between endothelial and smooth muscle cells in pulmonary hypertension: critical role for serotonin-induced smooth muscle hyperplasia. Circulation. 2006;113(15):1857–1864. doi: 10.1161/CIRCULATIONAHA.105.591321. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
