

Exosomes derived from smooth muscle cells ameliorate diabetes-induced erectile dysfunction by inhibiting fibrosis and modulating the NO/cGMP pathway
- PMID: 33009701
- PMCID: PMC7701535
- DOI: 10.1111/jcmm.15946
Exosomes derived from smooth muscle cells ameliorate diabetes-induced erectile dysfunction by inhibiting fibrosis and modulating the NO/cGMP pathway
Abstract
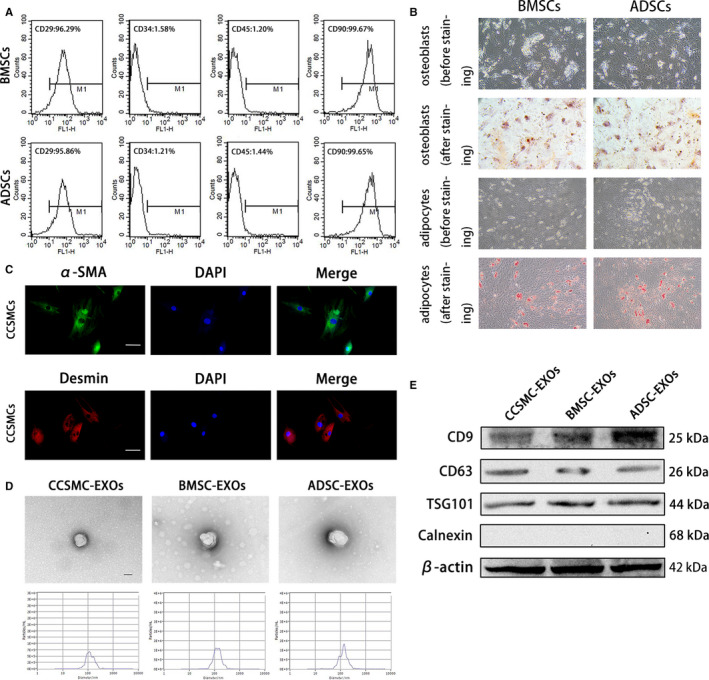
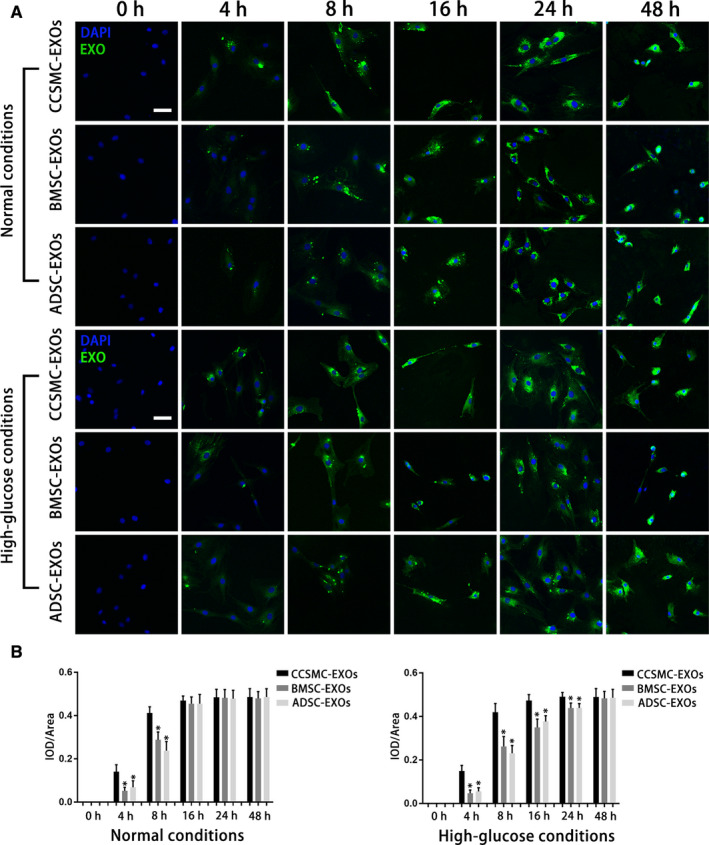
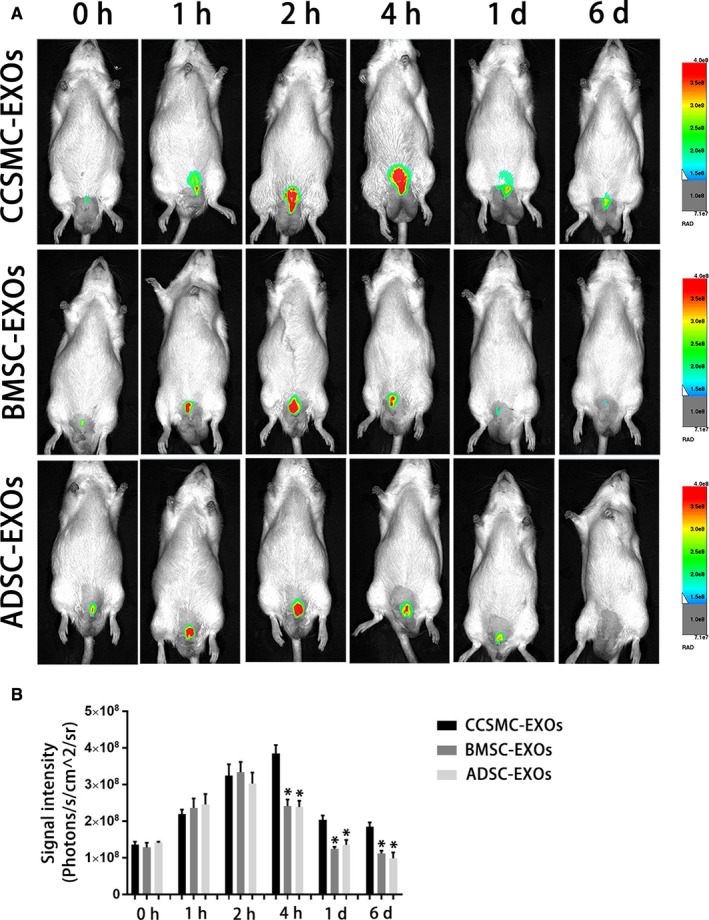
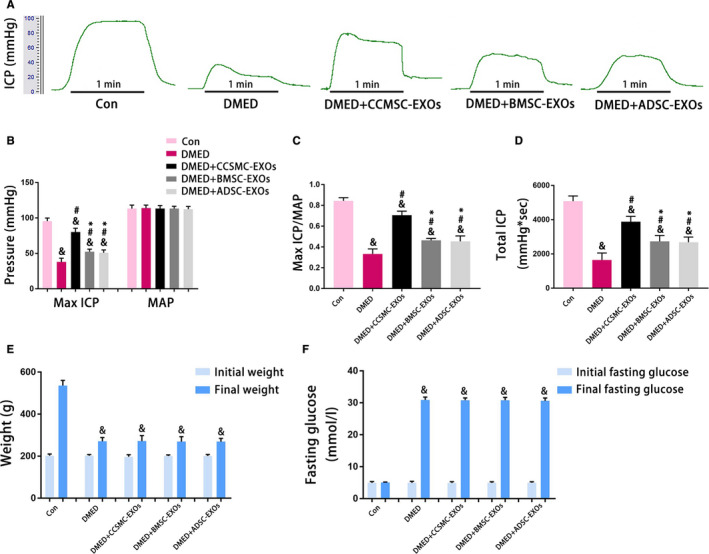
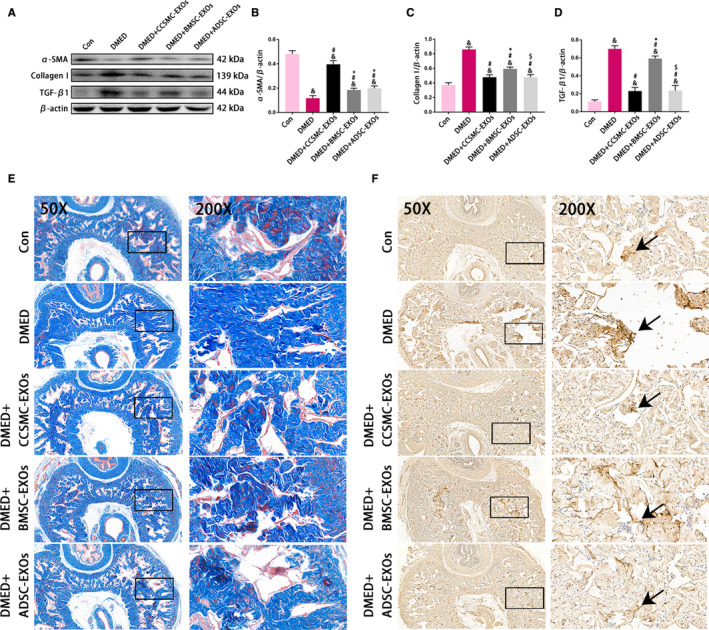
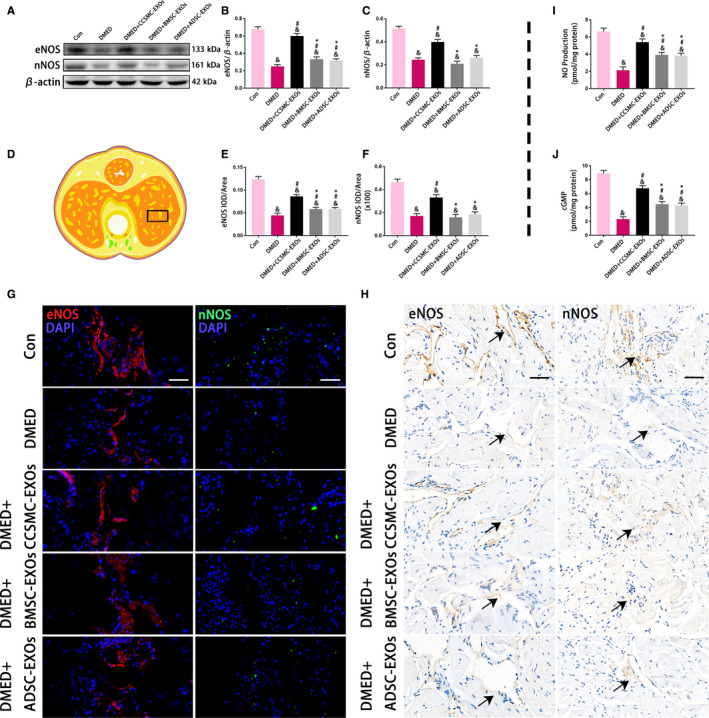
Erectile dysfunction (ED) is a major health issue among men with diabetes, and ED induced by diabetes mellitus (DMED) is particularly difficult to treat. Therefore, novel therapeutic approaches for the treatment of DMED are urgently needed. Exosomes, nanosized particles involved in many physiological and pathological processes, may become a promising tool for DMED treatment. In this study, we investigated the therapeutic effect of exosomes derived from corpus cavernosum smooth muscle cells (CCSMC-EXOs) on erectile function in a rat model of diabetes and compared their effect with that of exosomes derived from mesenchymal stem cells (MSC-EXOs). We incubated labelled CCSMC-EXOs and MSC-EXOs with CCSMCs and then observed uptake of the exosomes at different time points using laser confocal microscopy. CCSMC-EXOs were more easily taken up by CCSMCs. The peak concentration and retention time of labelled CCSMC-EXOs and MSC-EXOs in the corpus cavernosum of DMED rats after intracavernous injection were compared by in vivo imaging techniques. Intracavernous injection of CCSMC-EXOs was associated with a relatively high peak concentration and long retention time. Our data showed that CCSMC-EXOs could improve erectile function in DMED rats. Meanwhile, CCSMC-EXOs could exert antifibrotic effects by increasing the smooth muscle content and reducing collagen deposition. CCSMC-EXOs also increased the expression of eNOS and nNOS, followed by increased levels of NO and cGMP. These findings initially identify the possible role of CCSMC-EXOs in ameliorating DMED through inhibiting corporal fibrosis and modulating the NO/cGMP signalling pathway, providing a theoretical basis for a breakthrough in the treatment of DMED.
Keywords: NO/cGMP signalling pathway; diabetes; erectile dysfunction; exosomes; fibrosis.
© 2020 The Authors. Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
The authors confirm that there are no conflict of interest.
Figures
References
-
- Thorve VS, Kshirsagar AD, Vyawahare NS, Joshi VS, Ingale KG, Mohite RJ. Diabetes‐induced erectile dysfunction: epidemiology, pathophysiology and management. J Diabetes Complications. 2011;25:129‐136. - PubMed
-
- Shamloul R, Ghanem H. Erectile dysfunction. Lancet. 2013;381:153‐165. - PubMed
-
- Malavige LS, Levy JC. Erectile dysfunction in diabetes mellitus. J Sex Med. 2009;6:1232‐1247. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
