

Direct anterior versus posterior approach for total hip arthroplasty: a multicentre, prospective, randomized clinical trial
- PMID: 33009898
- PMCID: PMC7608717
- DOI: 10.1503/cjs.012019
Direct anterior versus posterior approach for total hip arthroplasty: a multicentre, prospective, randomized clinical trial
Abstract
Background: The ideal approach for a total hip arthroplasty (THA) would be kind to soft tissues, have the lowest complication rates and be easily reproducible. Although there have been several attempts to find the best approach for THA in the last decade, a definitive answer has not been found. We performed a prospective study to compare the direct anterior and posterior approaches for THA in terms of hospital length of stay, functional outcome, pain, implant position, complications and surgical time.
Methods: A prospective, randomized, multicentre clinical study was conducted between February 2011 and July 2013, with an average follow-up of 55 months. Patients undergoing the direct anterior or posterior approach for THA were enrolled. Hospital length of stay, surgical time and complications were documented. The Harris Hip Score and visual analogue scale were used to monitor functional outcome and pain until 5 years postoperatively. Radiologic analysis was used to assess implant position.
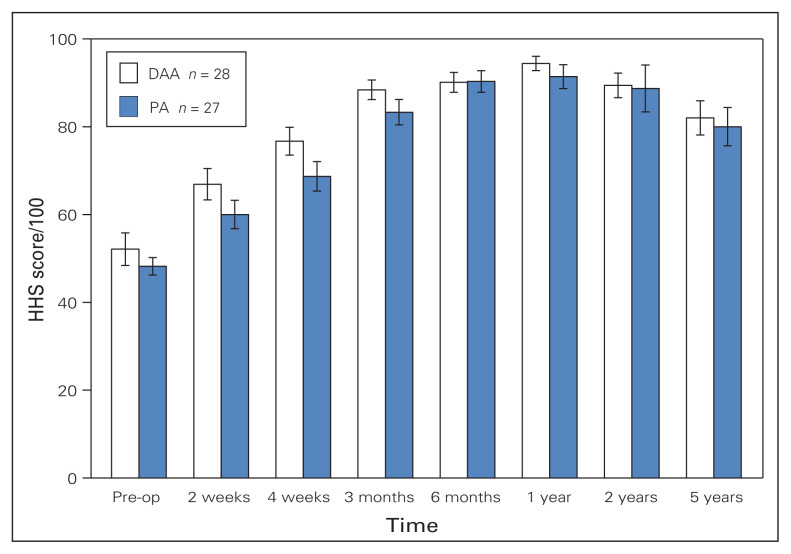
Results: Fifty-five patients (28 undergoing the direct anterior approach, 27 undergoing the posterior approach) were enrolled in this study. Length of stay, functional outcome, pain, implant position and complications were similar for the 2 approaches. There was a trend toward a better functional outcome for patients who underwent the direct anterior approach in the first 3 months postoperatively, with a peak at 4 weeks (Harris Hip Score 76.7 v. 68.7; p = 0.08). Average surgical time for the direct anterior approach was significantly longer (69.9 v. 45.7 min; p = 0.002).
Conclusion: The direct anterior approach for THA appears to be a safe and effective option. However, there is no significant difference in hospital length of stay or postoperative recovery between the 2 approaches.
Clinical trial registration: Clinicaltrials.gov, no. NCT03673514.
Contexte: L’approche idéale pour l’arthroplastie totale de la hanche (ATH) serait douce pour les tissus mous, aurait le taux de complications le plus bas et serait facilement reproductible. Dans les 10 dernières années, on a tenté à de nombreuses reprises de déterminer quelle est la meilleure approche, sans obtenir de réponse concluante. Nous avons mené une étude prospective visant à comparer la durée du séjour à l’hôpital, les résultats fonctionnels, la douleur, la position de l’implant, les complications et le temps de chirurgie associés aux approches antérieure directe et postérieure pour l’ATH.
Méthodes: Un essai clinique randomisé prospectif multicentrique a été mené auprès de patients ayant subi une ATH par voie antérieure directe ou postérieure entre février 2011 et juillet 2013; le suivi moyen était de 55 mois. La durée du séjour à l’hôpital, le temps de chirurgie et les complications ont été notés. Le score de Harris pour la hanche et l’échelle analogique visuelle ont servi au suivi des résultats fonctionnels et de la douleur dans les 5 ans suivant l’opération. Des clichés radiologiques ont été analysés pour évaluer la position de l’implant.
Résultats: Au total, 55 patients ont été recrutés (28 ayant subi une ATH par voie antérieure directe, et 27, une ATH par voie postérieure). La durée du séjour, les résultats fonctionnels, la douleur, la position de l’implant et les complications étaient sensiblement les mêmes, quelle que soit l’approche utilisée. Dans les 3 premiers mois suivant l’opération, les patients ayant subi une ATH par voie antérieure directe avaient tendance à présenter de meilleurs résultats fonctionnels que les autres, en particulier à la quatrième semaine postopératoire (score de Harris pour la hanche : 76,7 c. 68,7; p = 0,08). Le temps de chirurgie moyen pour l’approche antérieure directe était significativement plus long (69,9 c. 45,7 min; p = 0,002).
Conclusion: La voie antérieure directe semble être une approche efficace et sûre. Aucune différence significative n’a toutefois été observée entre les 2 approches quant à la durée du séjour à l’hôpital ou au rétablissement postopératoire.
Enregistrement de l’essai: ClinicalTrials.gov, no NCT03673514.
Conflict of interest statement
Figures
References
-
- Waddell J, Johnson K, Hein W, et al. Orthopaedic practice in total hip arthroplasty and total knee arthroplasty: results from the Global Orthopaedic Registry (GLORY) Am J Orthop. 2010;39(Suppl):5–13. - PubMed
-
- Chechik O, Khashan M, Lador R, et al. Surgical approach and prosthesis fixation in hip arthroplasty worldwide. Arch Orthop Trauma Surg. 2013;133:1595–600. - PubMed
-
- Kwon MS, Kuskowski M, Mulhall KJ, et al. Does surgical approach affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res. 2006;447:34–8. - PubMed
-
- Iorio R, Specht LM, Healy WL, et al. The effect of EPSTR and minimal incision surgery on dislocation after THA. Clin Orthop Relat Res. 2006;447:39–42. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical