

Dysregulated lipid metabolism links NAFLD to cardiovascular disease
- PMID: 33010471
- PMCID: PMC7600388
- DOI: 10.1016/j.molmet.2020.101092
Dysregulated lipid metabolism links NAFLD to cardiovascular disease
Abstract
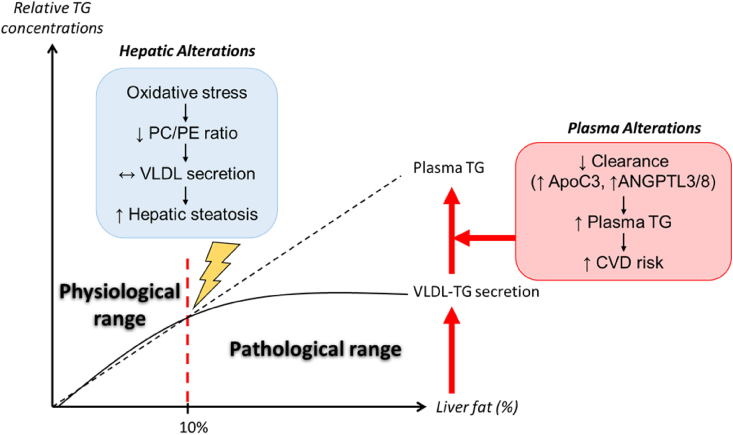
Background: Non-alcoholic fatty liver disease (NAFLD) is rapidly becoming a global health problem. Cardiovascular diseases (CVD) are the most common cause of mortality in NAFLD patients. NAFLD and CVD share several common risk factors including obesity, insulin resistance, and type 2 diabetes (T2D). Atherogenic dyslipidemia, characterized by plasma hypertriglyceridemia, increased small dense low-density lipoprotein (LDL) particles, and decreased high-density lipoprotein cholesterol (HDL-C) levels, is often observed in NAFLD patients.
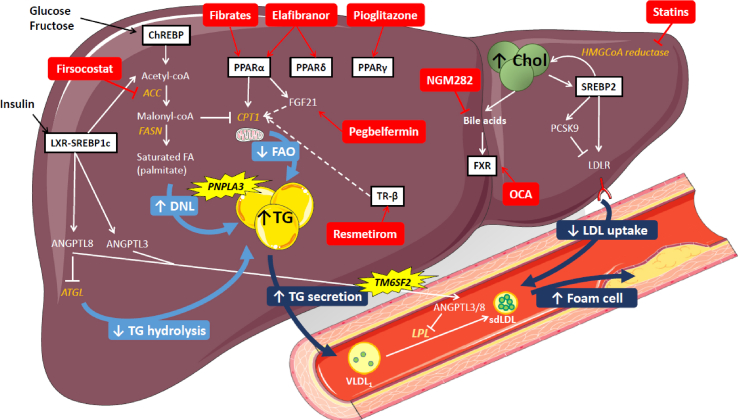
Scope of review: In this review, we highlight recent epidemiological studies evaluating the link between NAFLD and CVD risk. We further focus on recent mechanistic insights into the links between NAFLD and altered lipoprotein metabolism. We also discuss current therapeutic strategies for NAFLD and their potential impact on NAFLD-associated CVD risk.
Major conclusions: Alterations in hepatic lipid and lipoprotein metabolism are major contributing factors to the increased CVD risk in NAFLD patients, and many promising NASH therapies in development also improve dyslipidemia in clinical trials.
Keywords: Cardiovascular disease; Dyslipidemia; Metabolic syndrome; NAFLD.
Copyright © 2020 The Author(s). Published by Elsevier GmbH.. All rights reserved.
Figures
References
-
- Younossi Z.M., Koenig A.B., Abdelatif D., Fazel Y., Henry L., Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. - PubMed
-
- Haas J.T., Francque S., Staels B. Pathophysiology and mechanisms of nonalcoholic fatty liver disease. Annual Review of Physiology. 2016;78:181–205. - PubMed
-
- Eslam M., Sanyal A.J., George J., International Consensus Panel MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
