

Surgical treatment of femoral head fractures
- PMID: 33011107
- PMCID: PMC7680813
- DOI: 10.1016/j.bj.2019.08.004
Surgical treatment of femoral head fractures
Abstract
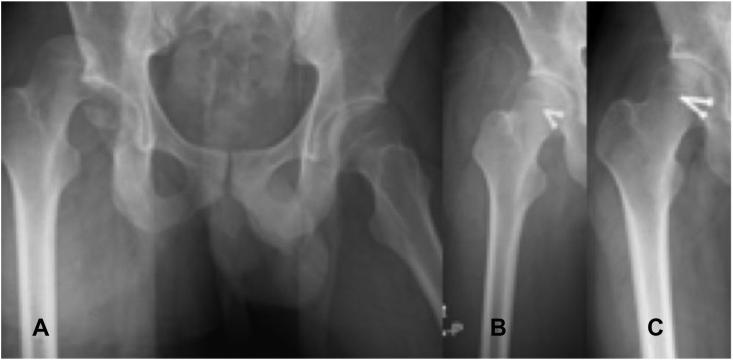
Background: Femoral head fractures (FHF) are uncommon and generally caused by high-energy injuries. Surgical reduction with stable fixation of large fragments is believed to have the best outcomes. This retrospective study intended to report outcomes with surgical treatment at our institution and tried to establish treatment algorithm.
Methods: Through the 6-year period (2003-2008), 35 FHF in 35 consecutive patients (average, 30 years) were surgically treated. All FHF were caused by high-energy trauma. Patients' general condition was stabilized first and hip dislocation was manually reduced immediately. Definite fracture treatment was scheduled after admission for an average of 2.9 days (0.3-11 days). Pipkin classification was used as the treatment guide and open reduction with internal fixation was performed in all 35 FHF.
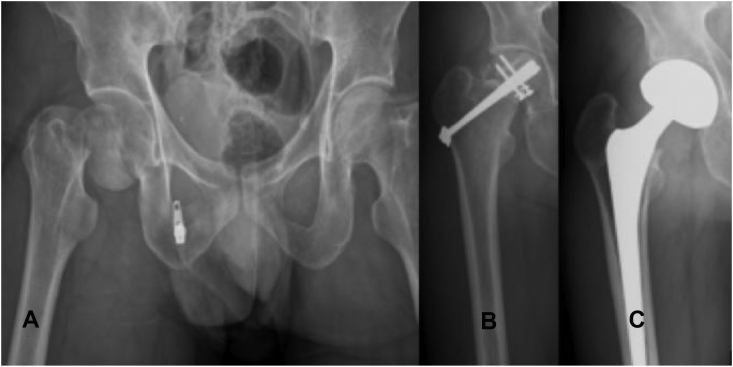
Results: These FHF included 21 type I, 7 type II, 3 type III, and 4 type IV fractures. The hip joint had been approached by either an anterior or posterior route depending on the individual surgeon. Internal fixation with screws was performed for all 35 FHF. The average admission was 13.8 days (range, 2-35 days). Thirty patients (86%, 30/35) were followed for an average of 3.3 years (at lease 6 months) and all 30 FHF healed. Avascular necrosis of the femoral head was found in 23% (7/30) patients and six patients were converted to hip arthroplasty for developing advanced stages of avascular necrosis. Heterotopic ossification occurred in 43% (13/30) patients. However, only one patient had range of motion limitation. Besides, one patient had moderate hip osteoarthritis.
Conclusions: FHF are uncommon and generally caused by high-energy injuries. Fracture healing can be attained in all femoral head fractures by using open reduction and screw fixation. Our results by using conventional approaches were associated with high complication rates. Further endeavor to improve the outcome should be taken.
Keywords: Avascular necrosis; Femoral head fracture; Heterotopic ossification; Internal fixation; Osteoarthritis.
Copyright © 2019 Chang Gung University. Published by Elsevier B.V. All rights reserved.
Figures


References
-
- Droll K.P., Broekhuyse H., O'Brien P. Fracture of the femoral head. J Am Acad Orthop Surg. 2007;15:716–727. - PubMed
-
- Henle P., Kloen P., Siebenrock K.A. Femoral head injuries: which treatment strategy can be recommended? Injury. 2007;38:478–488. - PubMed
-
- Hankin M.H., Morse D.E., Bennett-Clerke C.A. McGraw-Hill Medical; New York, NY: 2013. Clinical anatomy: a case study approach; pp. 350–355.
-
- Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957;39:1027–1042. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
