

Fecal Microbiota Transplantation Is Highly Effective in Real-World Practice: Initial Results From the FMT National Registry
- PMID: 33011173
- PMCID: PMC8034505
- DOI: 10.1053/j.gastro.2020.09.038
Fecal Microbiota Transplantation Is Highly Effective in Real-World Practice: Initial Results From the FMT National Registry
Abstract
Background & aims: Fecal microbiota transplantation (FMT) is used commonly for treatment of Clostridioides difficile infections (CDIs), although prospective safety data are limited and real-world FMT practice and outcomes are not well described. The FMT National Registry was designed to assess FMT methods and both safety and effectiveness outcomes from North American FMT providers.
Methods: Patients undergoing FMT in clinical practices across North America were eligible. Participating investigators enter de-identified data into an online platform, including FMT protocol, baseline patient characteristics, CDI cure and recurrence, and short and long-term safety outcomes.
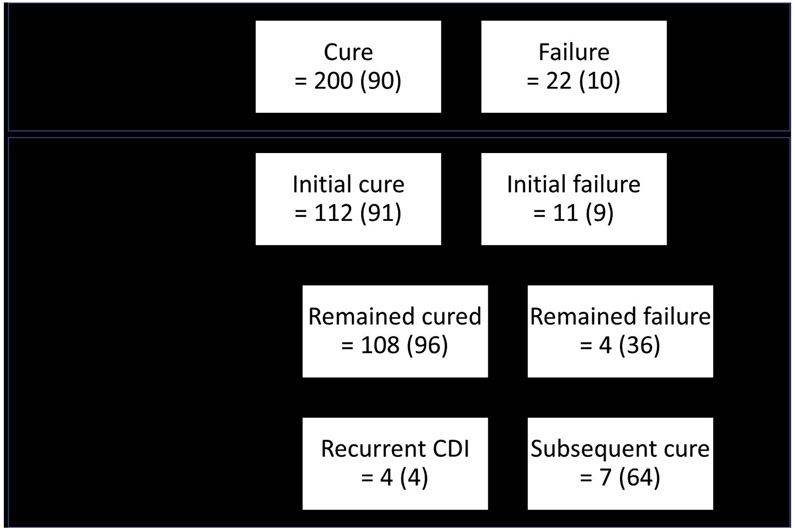
Results: Of the first 259 participants enrolled at 20 sites, 222 had completed short-term follow-up at 1 month and 123 had follow-up to 6 months; 171 (66%) were female. All FMTs were done for CDI and 249 (96%) used an unknown donor (eg, stool bank). One-month cure occurred in 200 patients (90%); of these, 197 (98%) received only 1 FMT. Among 112 patients with initial cure who were followed to 6 months, 4 (4%) had CDI recurrence. Severe symptoms reported within 1-month of FMT included diarrhea (n = 5 [2%]) and abdominal pain (n = 4 [2%]); 3 patients (1%) had hospitalizations possibly related to FMT. At 6 months, new diagnoses of irritable bowel syndrome were made in 2 patients (1%) and inflammatory bowel disease in 2 patients (1%).
Conclusions: This prospective real-world study demonstrated high effectiveness of FMT for CDI with a good safety profile. Assessment of new conditions at long-term follow-up is planned as this registry grows and will be important for determining the full safety profile of FMT.
Keywords: Bacteriotherapy; Microbiome; Risk.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Conflicts of interest
These authors disclose the following: Colleen R. Kelly: research support from Finch Therapeutics for a clinical trial; unpaid clinical advisor to OpenBiome. Ari M. Grinspan: lecture fees from Merck. Stacy A. Kahn: unpaid research collaboration with OpenBiome; pilot award (principal investigator) from Cures Within Reach; Mooney Fund Research Award (principal investigator). James D. Lewis: consulting for Merck and Pfizer, outside of submitted work. David T. Rubin: no disclosures relevant to the submitted work, but has received research support from Takeda and serves as a consultant for Abbvie, Abgenomics, Allergan, Inc, Arena Pharmaceuticals, Biomica, Bristol-Myers Squibb, Dizal Pharmaceuticals, Ferring Pharmaceuticals, Inc, Genentech/ Roche, Janssen Pharmaceuticals, Lilly, Mahana Therapeutics, Medtronic, Merck & Co., Inc, Napo Pharmaceuticals, Pfizer, Prometheus Laboratories, Shire, Takeda, and Target PharmaSolutions, Inc. Jessica R. Allegretti: consults for Finch Therapeutics, Servatus, and Artugen and is an unpaid advisor to Openbiome. Jessica R. Allegretti has research support from Merck. Sahil Khanna: research grants from Rebiotix, Inc (A Ferring Company), consulting fees from Shire Plc, Premier Inc, Facile therapeutics, ProbioTech Inc, outside of the submitted work. Carl V. Crawford: research support from Finch Therapeutics, Summit, Ferring, and Artugen for clinical trials. Speaker for Merck and Romark. Monika Fischer: on data and safety monitoring board for Rebiotix; unpaid clinical advisor to OpenBiome. Paul Feuerstadt: consulting fees for Merck and Co., Rebiotix (A Ferring Company), Roche Diagnostics and Premier Inc David Kerman: Consultant to Abbvie, Cleveland Clinic, Advisory Board Rebiotix. Jonathan Goldstein: research support from Rebiotix. Gary D. Wu: research support from Intercept Pharmaceuticals, Seres Therapeutics, and Takeda Pharmaceuticals; scientific consultant for the Hitachi Corporation; and a scientific advisory board member for Biocodex and Danone. The remaining authors disclose no conflicts.
Figures
Comment in
-
Fecal Microbiota Transplantation "Donor Effects" Are Not Clinically Relevant for Clostridioides difficile Infection.Gastroenterology. 2021 Jun;160(7):2635-2636. doi: 10.1053/j.gastro.2020.12.057. Epub 2020 Dec 30. Gastroenterology. 2021. PMID: 33387515 No abstract available.
-
Reply.Gastroenterology. 2021 Jun;160(7):2636. doi: 10.1053/j.gastro.2021.02.045. Epub 2021 Feb 25. Gastroenterology. 2021. PMID: 33639155 No abstract available.
References
-
- Ma GK, Brensinger CM, Wu Q, et al. Increasing incidence of multiply recurrent clostridium difficile infection in the United States: a cohort study. Ann Intern Med 2017; 167:152–158. - PubMed
-
- McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol 2002; 97:1769–1775. - PubMed
-
- Moayyedi P, Yuan Y, Baharith H, et al. Faecal microbiota transplantation for Clostridium difficile-associated diarrhoea: a systematic review of randomised controlled trials. Med J Aust 2017;207:166–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
