

Deep learning-based digitization of prostate brachytherapy needles in ultrasound images
- PMID: 33012023
- PMCID: PMC7821271
- DOI: 10.1002/mp.14508
Deep learning-based digitization of prostate brachytherapy needles in ultrasound images
Abstract
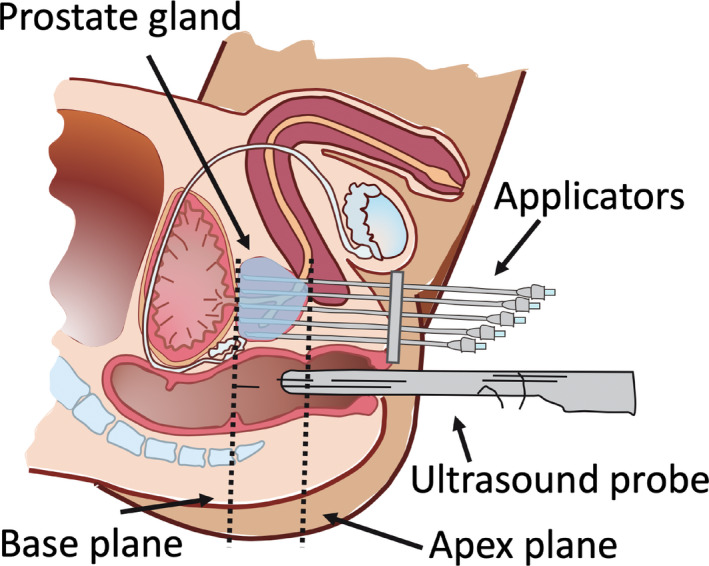
Purpose: To develop, and evaluate the performance of, a deep learning-based three-dimensional (3D) convolutional neural network (CNN) artificial intelligence (AI) algorithm aimed at finding needles in ultrasound images used in prostate brachytherapy.
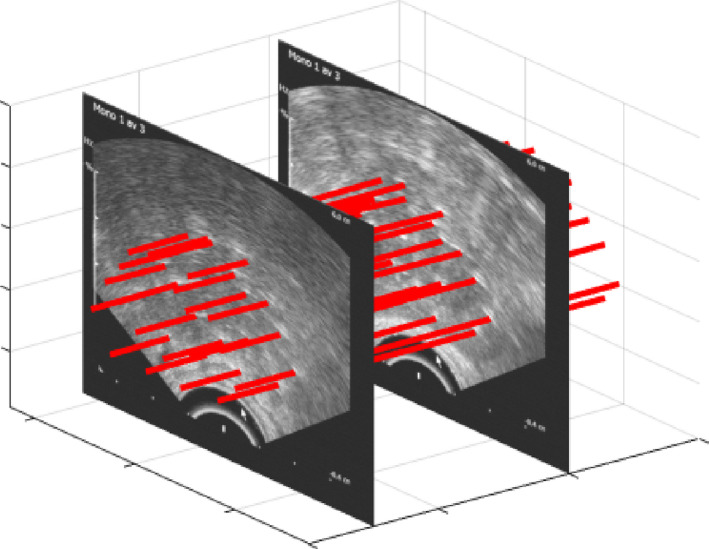
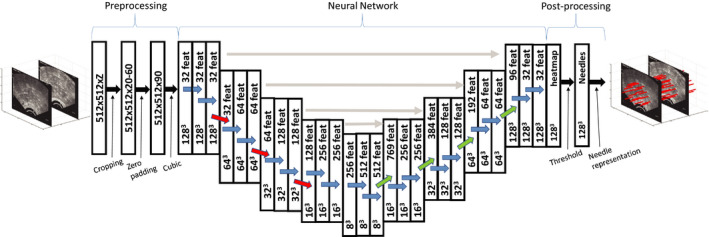
Methods: Transrectal ultrasound (TRUS) image volumes from 1102 treatments were used to create a clinical ground truth (CGT) including 24422 individual needles that had been manually digitized by medical physicists during brachytherapy procedures. A 3D CNN U-net with 128 × 128 × 128 TRUS image volumes as input was trained using 17215 needle examples. Predictions of voxels constituting a needle were combined to yield a 3D linear function describing the localization of each needle in a TRUS volume. Manual and AI digitizations were compared in terms of the root-mean-square distance (RMSD) along each needle, expressed as median and interquartile range (IQR). The method was evaluated on a data set including 7207 needle examples. A subgroup of the evaluation data set (n = 188) was created, where the needles were digitized once more by a medical physicist (G1) trained in brachytherapy. The digitization procedure was timed.
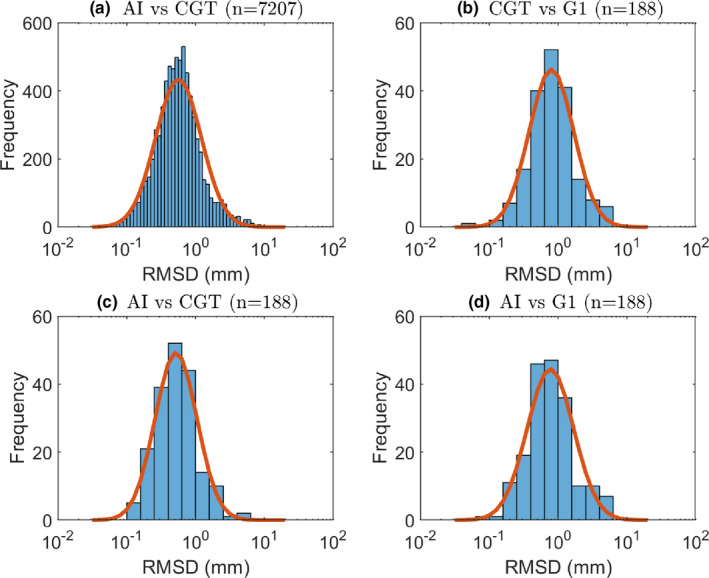
Results: The RMSD between the AI and CGT was 0.55 (IQR: 0.35-0.86) mm. In the smaller subset, the RMSD between AI and CGT was similar (0.52 [IQR: 0.33-0.79] mm) but significantly smaller (P < 0.001) than the difference of 0.75 (IQR: 0.49-1.20) mm between AI and G1. The difference between CGT and G1 was 0.80 (IQR: 0.48-1.18) mm, implying that the AI performed as well as the CGT in relation to G1. The mean time needed for human digitization was 10 min 11 sec, while the time needed for the AI was negligible.
Conclusions: A 3D CNN can be trained to identify needles in TRUS images. The performance of the network was similar to that of a medical physicist trained in brachytherapy. Incorporating a CNN for needle identification can shorten brachytherapy treatment procedures substantially.
Keywords: brachytherapy; deep learning; high-dose-rate; image segmentation; needle digitization.
© 2020 The Authors. Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflict to disclose.
Figures
Similar articles
-
Multi-needle Localization with Attention U-Net in US-guided HDR Prostate Brachytherapy.Med Phys. 2020 Jul;47(7):2735-2745. doi: 10.1002/mp.14128. Epub 2020 Apr 3. Med Phys. 2020. PMID: 32155666 Free PMC article.
-
Deep learning-based ultrasound auto-segmentation of the prostate with brachytherapy implanted needles.Med Phys. 2024 Apr;51(4):2665-2677. doi: 10.1002/mp.16811. Epub 2023 Oct 27. Med Phys. 2024. PMID: 37888789
-
Automatic prostate segmentation using deep learning on clinically diverse 3D transrectal ultrasound images.Med Phys. 2020 Jun;47(6):2413-2426. doi: 10.1002/mp.14134. Epub 2020 Apr 8. Med Phys. 2020. PMID: 32166768
-
Use of three-dimensional radiation therapy planning tools and intraoperative ultrasound to evaluate high dose rate prostate brachytherapy implants.Int J Radiat Oncol Biol Phys. 1999 Feb 1;43(3):571-8. doi: 10.1016/s0360-3016(98)00420-9. Int J Radiat Oncol Biol Phys. 1999. PMID: 10078639 Review.
-
Clinical evaluation of an MRI-to-ultrasound deformable image registration algorithm for prostate brachytherapy.Brachytherapy. 2019 Jan-Feb;18(1):95-102. doi: 10.1016/j.brachy.2018.08.006. Epub 2018 Oct 2. Brachytherapy. 2019. PMID: 30287271 Review.
Cited by
-
Bridging the simulation-to-real gap for AI-based needle and target detection in robot-assisted ultrasound-guided interventions.Eur Radiol Exp. 2023 Jun 19;7(1):30. doi: 10.1186/s41747-023-00344-x. Eur Radiol Exp. 2023. PMID: 37332035 Free PMC article.
-
Artificial intelligence in interventional radiotherapy (brachytherapy): Enhancing patient-centered care and addressing patients' needs.Clin Transl Radiat Oncol. 2024 Sep 22;49:100865. doi: 10.1016/j.ctro.2024.100865. eCollection 2024 Nov. Clin Transl Radiat Oncol. 2024. PMID: 39381628 Free PMC article. Review.
-
Attention-Gated Deep-Learning-Based Automatic Digitization of Interstitial Needles in High-Dose-Rate Brachytherapy for Cervical Cancer.Adv Radiat Oncol. 2023 Aug 10;9(1):101340. doi: 10.1016/j.adro.2023.101340. eCollection 2024 Jan. Adv Radiat Oncol. 2023. PMID: 38260236 Free PMC article.
-
Deep-learning-assisted algorithm for catheter reconstruction during MR-only gynecological interstitial brachytherapy.J Appl Clin Med Phys. 2022 Feb;23(2):e13494. doi: 10.1002/acm2.13494. Epub 2021 Dec 10. J Appl Clin Med Phys. 2022. PMID: 34889509 Free PMC article.
-
Ultrasound-guided needle tracking with deep learning: A novel approach with photoacoustic ground truth.Photoacoustics. 2023 Nov 29;34:100575. doi: 10.1016/j.pacs.2023.100575. eCollection 2023 Dec. Photoacoustics. 2023. PMID: 38174105 Free PMC article.
References
-
- Hoskin PJ, Colombo A, Henry A, et al. GEC/ESTRO recommendations on high dose rate afterloading brachytherapy for localised prostate cancer: an update. Radiother Oncol. 2013;107:325–332. - PubMed
-
- Bentzen JK, Ockelmann HH, Hansen HS. [High dose rate 192Ir‐Microselectron]. Ugeskr . Laeg. 1990;152:2908–2910. - PubMed
-
- Milickovic N, Tselis N, Karagiannis E, Ferentinos K, Zamboglou N. Iridium‐knife: another knife in radiation oncology. Brachytherapy. 2017;16:884–892. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
