

Quantification of Aerosol Particle Concentrations During Endoscopic Sinonasal Surgery in the Operating Room
- PMID: 33012174
- PMCID: PMC8822194
- DOI: 10.1177/1945892420962335
Quantification of Aerosol Particle Concentrations During Endoscopic Sinonasal Surgery in the Operating Room
Abstract
Background: Recent indirect evidence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) transmission during endoscopic endonasal procedures has highlighted the dearth of knowledge surrounding aerosol generation with these procedures. As we adapt to function in the era of Coronavirus Disease 2019 (COVID-19) a better understanding of how surgical techniques generate potentially infectious aerosolized particles will enhance the safety of operating room (OR) staff and learners.
Objective: To provide greater understanding of possible SARS-CoV-2 exposure risk during endonasal surgeries by quantifying increases in airborne particle concentrations during endoscopic sinonasal surgery.
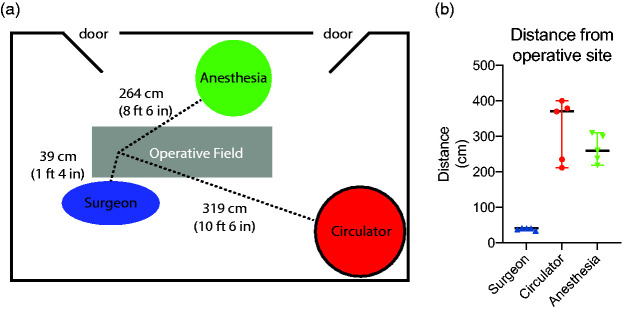
Methods: Aerosol concentrations were measured during live-patient endoscopic endonasal surgeries in ORs with an optical particle sizer. Measurements were taken throughout the procedure at six time points: 1) before patient entered the OR, 2) before pre-incision timeout during OR setup, 3) during cold instrumentation with suction, 4) during microdebrider use, 5) during drill use and, 6) at the end of the case prior to extubation. Measurements were taken at three different OR position: surgeon, circulating nurse, and anesthesia provider.
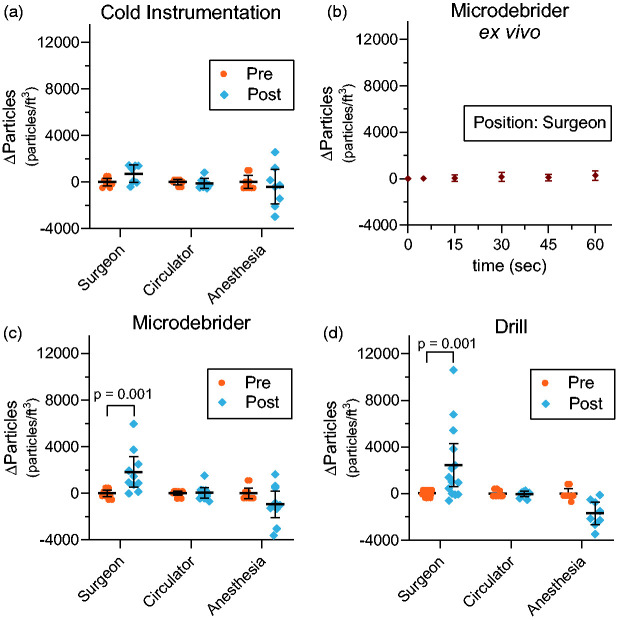
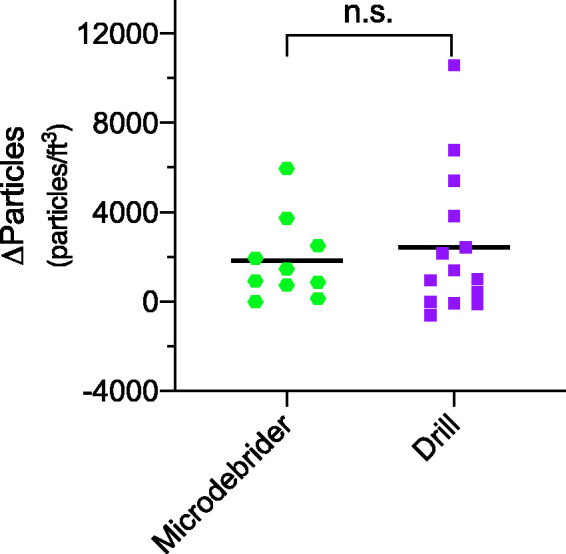
Results: Significant increases in airborne particle concentration were measured at the surgeon position with both the microdebrider (p = 0.001) and drill (p = 0.001), but not for cold instrumentation with suction (p = 0.340). Particle concentration did not significantly increase at the anesthesia position or the circulator position with any form of instrumentation. Overall, the surgeon position had a mean increase in particle concentration of 2445 particles/ft3 (95% CI 881 to 3955; p = 0.001) during drill use and 1825 particles/ft3 (95% CI 641 to 3009; p = 0.001) during microdebrider use.
Conclusion: Drilling and microdebrider use during endonasal surgery in a standard operating room is associated with a significant increase in airborne particle concentrations. Fortunately, this increase in aerosol concentration is localized to the area of the operating surgeon, with no detectable increase in aerosol particles at other OR positions.
Keywords: COVID-19; SARS-CoV-2; aerosolization; airborne particles; endoscopic sinus surgery.
Conflict of interest statement
Figures
Similar articles
-
Quantification of Aerosol Concentrations During Endonasal Instrumentation in the Clinic Setting.Laryngoscope. 2021 May;131(5):E1415-E1421. doi: 10.1002/lary.29122. Epub 2020 Oct 5. Laryngoscope. 2021. PMID: 33017067 Free PMC article.
-
Endonasal instrumentation and aerosolization risk in the era of COVID-19: simulation, literature review, and proposed mitigation strategies.Int Forum Allergy Rhinol. 2020 Jul;10(7):798-805. doi: 10.1002/alr.22577. Epub 2020 May 22. Int Forum Allergy Rhinol. 2020. PMID: 32243678
-
Airborne Aerosol Generation During Endonasal Procedures in the Era of COVID-19: Risks and Recommendations.Otolaryngol Head Neck Surg. 2020 Sep;163(3):465-470. doi: 10.1177/0194599820931805. Epub 2020 May 26. Otolaryngol Head Neck Surg. 2020. PMID: 32452739 Free PMC article.
-
Are urologists in trouble with SARS-CoV-2? Reflections and recommendations for specific interventions.BJU Int. 2020 Dec;126(6):670-678. doi: 10.1111/bju.15141. Epub 2020 Aug 17. BJU Int. 2020. PMID: 32562351 Free PMC article. Review.
-
Diagnostic and therapeutic endonasal rhinologic procedures generating aerosol during COVID-19 pandemic: a systematized review.Braz J Otorhinolaryngol. 2021 Jul-Aug;87(4):469-477. doi: 10.1016/j.bjorl.2020.11.008. Epub 2020 Dec 13. Braz J Otorhinolaryngol. 2021. PMID: 33358322 Free PMC article.
Cited by
-
COVID-19 Testing in the Era of Modern Neurosurgery: Mitigating Risk in Our Vulnerable Patient Populations.World Neurosurg. 2021 Aug;152:80-83. doi: 10.1016/j.wneu.2021.06.027. Epub 2021 Jun 13. World Neurosurg. 2021. PMID: 34133996 Free PMC article.
-
Experimental study on the exposure level of surgical staff to SARS-CoV-2 in operating rooms with mixing ventilation under negative pressure.Build Environ. 2022 Jun 1;217:109091. doi: 10.1016/j.buildenv.2022.109091. Epub 2022 Apr 21. Build Environ. 2022. PMID: 35469260 Free PMC article.
-
Are medical procedures that induce coughing or involve respiratory suctioning associated with increased generation of aerosols and risk of SARS-CoV-2 infection? A rapid systematic review.J Hosp Infect. 2021 Oct;116:37-46. doi: 10.1016/j.jhin.2021.06.011. Epub 2021 Jul 8. J Hosp Infect. 2021. PMID: 34245806 Free PMC article.
-
Follow-up of a national web-based survey on the SARS-CoV-2 infectious state of otorhinolaryngologists in Germany.HNO. 2021 Aug;69(8):658-665. doi: 10.1007/s00106-021-01075-4. Epub 2021 Jun 4. HNO. 2021. PMID: 34086058 Free PMC article.
-
Surgical Management of Inferior Turbinate Hypertrophy in the Era of Widespread Communicable Disease.Cureus. 2023 Jan 27;15(1):e34280. doi: 10.7759/cureus.34280. eCollection 2023 Jan. Cureus. 2023. PMID: 36855496 Free PMC article. Review.
References
-
- Livingston E, Desai A, Berkwits M. Sourcing personal protective equipment during the COVID-19 pandemic. JAMA. 2020; 323(19):1912–1914. - PubMed
-
- Nacoti M, Ciocca A, Giupponi A. At the epicenter of the Covid-19 pandemic and humanitarian crises in Italy: changing perspectives on preparation and mitigation. NEJM Catal Innov Care Deliv. 2020; 1(2).
-
- Abbasi J. The promise and peril of antibody testing for COVID-19. JAMA. 2020; 323(19):1881–1883. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
