

Anatomic Suitability for Branched Thoracic Endovascular Repair in Patients with Aortic Arch Pathological Features
- PMID: 33012240
- PMCID: PMC7763389
- DOI: 10.1161/JAHA.120.016695
Anatomic Suitability for Branched Thoracic Endovascular Repair in Patients with Aortic Arch Pathological Features
Abstract
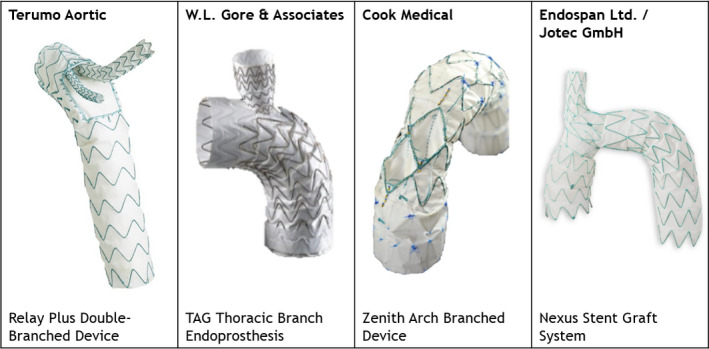
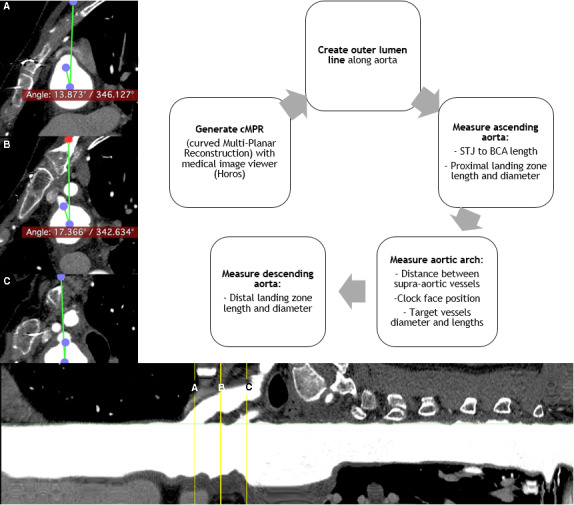
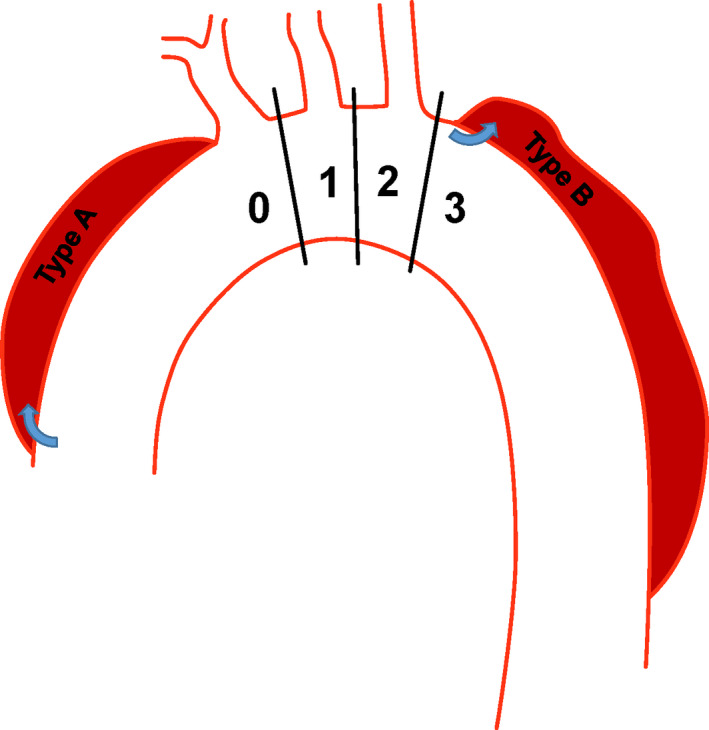
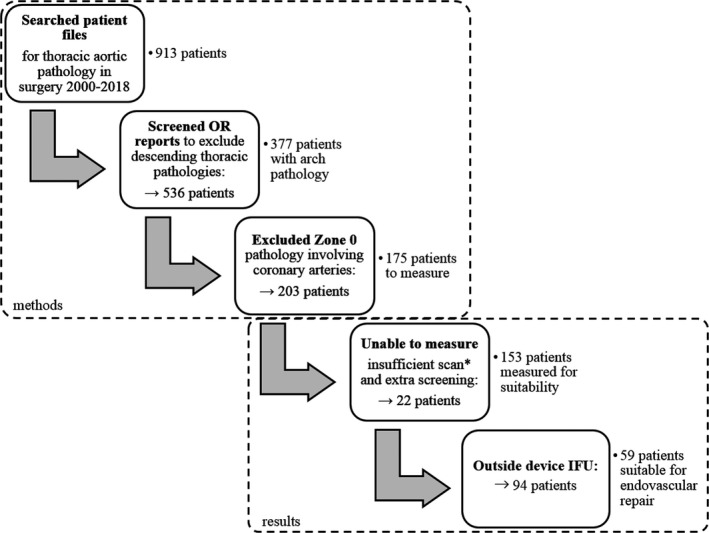
Background Endovascular repair has become a viable alternative for aortic pathological features, including those located within the aortic arch. We investigated the anatomic suitability for branched thoracic endovascular repair in patients previously treated with conventional open surgery for aortic arch pathological features. Methods and Results Patients who underwent open surgery for aortic arch pathological features at our institution between 2000 and 2018 were included. Anatomic suitability was determined by strict compliance with the anatomic criteria within manufacturers' instructions for use for each of the following branched thoracic stent grafts: Relay Plus Double-Branched (Terumo-Aortic), TAG Thoracic Branch Endoprosthesis (W.L. Gore & Associates), Zenith Arch Branched Device (Cook-Medical), and Nexus Stent Graft System (Endospan Ltd/Jotec GmbH). Computed tomography angiography images were analyzed with outer luminal line measurements. A total of 377 patients (mean age, 64±14 years; 64% men) were identified, 153 of whom had suitable computed tomography angiography images for measurements. In total, 59 patients (15.6% of the total cohort and 38.6% of the measured cohort) were eligible for endovascular repair using at least one of the devices. Device suitability was 30.9% for thoracic aneurysms, 4.6% for type A dissections, 62.5% for type B dissections, and 28.6% for other pathological features. Conclusions The anatomic suitability for endovascular repair of all aortic arch pathological features was modest. The highest suitability rates were observed for thoracic aneurysms and for type B dissections, of which repair included part of the aortic arch. We suggest endovascular repair of arch pathological features should be reserved for high-volume centers with experience in endovascular arch repair.
Keywords: anatomic suitability; aortic arch; branched stent grafts; cardiothoracic surgery; novel treatment; thoracic endovascular repair; vascular surgery.
Conflict of interest statement
None.
Figures
References
-
- Sundt TM 3rd, Orszulak TA, Cook DJ, Schaff HV. Improving results of open arch replacement. Ann Thorac Surg. 2008;787–796. - PubMed
-
- Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, Evangelista A, Fattori R, Suzuki T, Oh JK, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;897–903. - PubMed
-
- Girsowicz E, Georg Y, Lefebvre F, Lejay A, Thaveau F, Roy C, Ohana M, Chakfe N. Anatomical study of healthy aortic arches. Ann Vasc Surg. 2017;179–189. - PubMed
-
- Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent‐grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med. 1994;1729–1734. - PubMed
-
- Vallabhajosyula P, Szeto WY. Current paradigms in aortic arch repair: striking the balance between open surgery and endovascular repair. J Thorac Cardiovasc Surg. 2015;1399–1400. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
