

The Impact of the Support, Educate, Empower Personalized Glaucoma Coaching Pilot Study on Glaucoma Medication Adherence
- PMID: 33012330
- PMCID: PMC7528849
- DOI: 10.1016/j.ogla.2020.04.013
The Impact of the Support, Educate, Empower Personalized Glaucoma Coaching Pilot Study on Glaucoma Medication Adherence
Abstract
Purpose: To assess the efficacy of the Support, Educate, Empower (SEE) glaucoma coaching program on medication adherence among glaucoma patients with low adherence.
Design: Uncontrolled intervention study with a pre-post design.
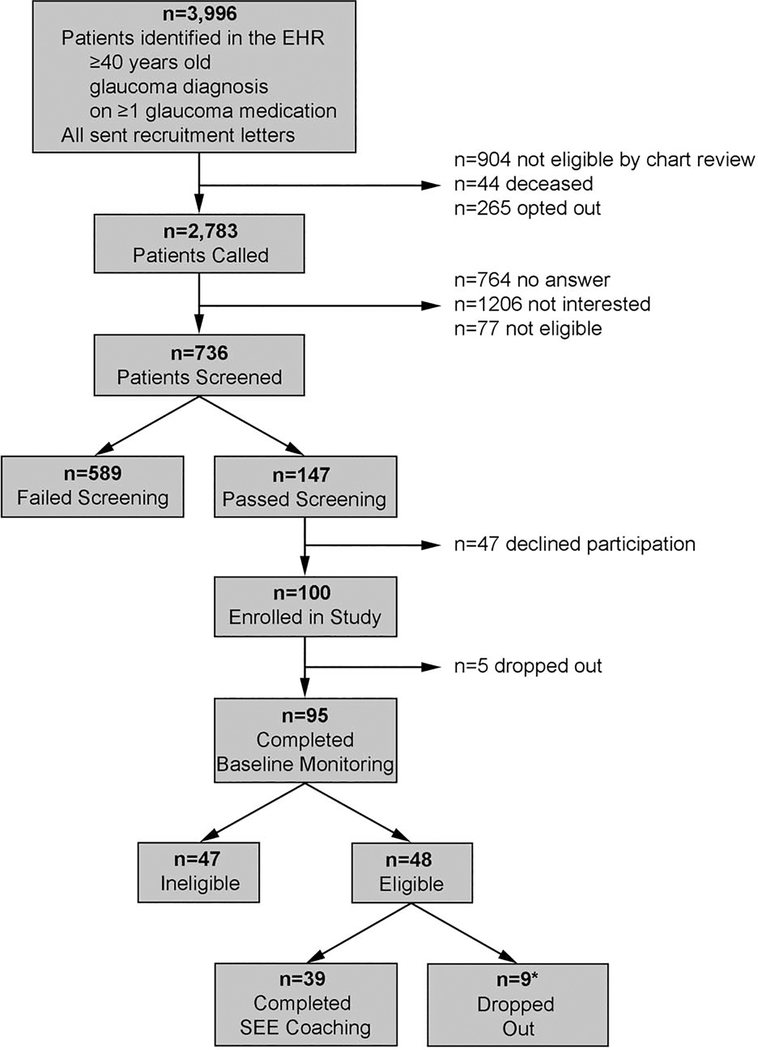
Participants: Glaucoma patients ≥ age 40, taking ≥1 medication, who self-reported poor adherence were recruited from the University of Michigan Kellogg Eye Center. Adherence was monitored electronically for a 3-month baseline period; participants with median adherence of ≤80% were enrolled in the SEE program.
Methods: Participants' adherence was monitored electronically (AdhereTech, New York, NY) during the 7-month program. Adherence was calculated as the percentage of doses taken on time of those prescribed. The SEE program included (1) automated medication reminders, (2) 3 in-person counseling sessions with a glaucoma coach who had training in motivational interviewing (MI), and (3) 5 phone calls with the same coach for between-session support. The coach used a web-based tool to generate an education plan tailored to the patient's glaucoma diagnosis, test results, and ophthalmologist's recommendations (www.glaucomaeyeguide.org). The tool guided an MI-based conversation between coach and patient to identify barriers to adherence and possible solutions. Descriptive statistics were used to summarize baseline patient characteristics, and differences between those who did and did not complete the SEE program were tested with 2-sample t tests, chi-square tests, and Fisher exact tests. Adherence was compared before and after the SEE program with paired t tests.
Main outcome measure: Change in electronically monitored medication adherence.
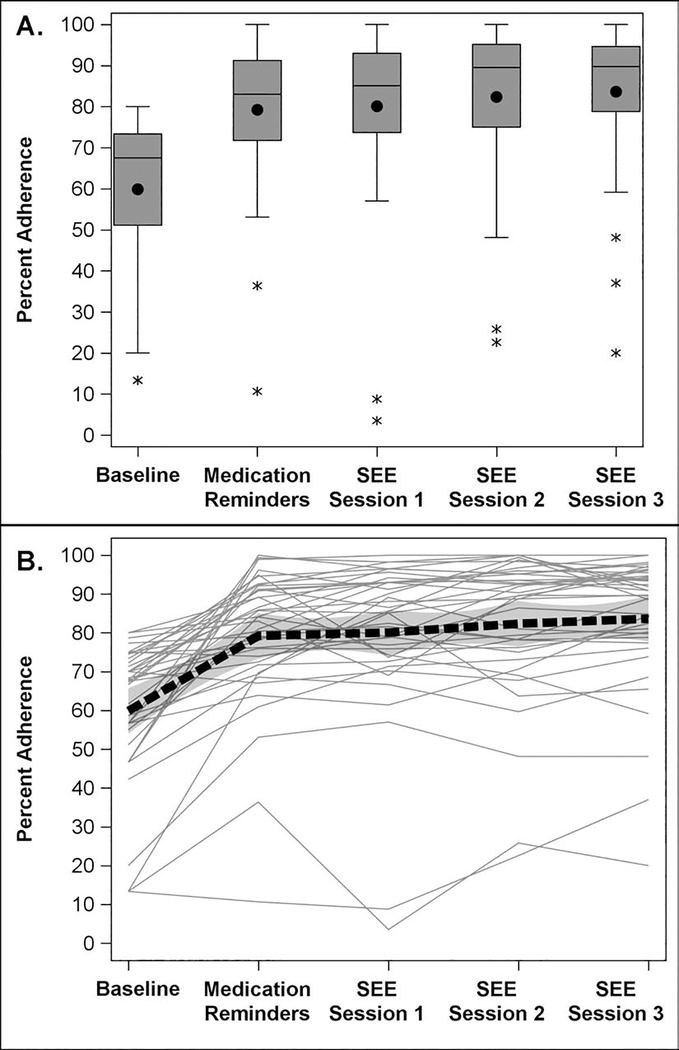
Results: A total of 48 participants were enrolled. The participants were 54% male, 46% white, and on average 64 years of age (standard deviation [SD], 10.8 years), with an average worse-eye mean deviation (MD) of -7.9 dB (SD, 8.8 dB). Those completing the SEE program (n = 39) did not differ significantly from those who dropped out (n = 9) on gender, race, age, MD, or baseline adherence. Medication adherence improved from 59.9% at baseline to 81.3% (P < 0.0001) after completing the SEE program. Ninety-five percent of participants showed an improvement in adherence (mean relative improvement, 21.4%; SD, 16.5%; range, -3.2% to 74.4%; median, 20.1%). Fifty-nine percent of participants showed adherence of >80% on completing the SEE program.
Conclusions: The SEE program participants showed clinically meaningful, statistically significant improvement in glaucoma medication adherence.
Copyright © 2020 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: No conflicting relationships exist for any author.
Figures
Comment in
-
Adherence Studies with Short Follow-up Do Not Suffice for a Chronic Disease Like Open-Angle Glaucoma.Ophthalmol Glaucoma. 2020 Jul-Aug;3(4):225-227. doi: 10.1016/j.ogla.2020.05.007. Epub 2020 Jul 23. Ophthalmol Glaucoma. 2020. PMID: 33008555 No abstract available.
References
-
- Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Heal. 2013;1:e339–e349. - PubMed
-
- World Health Organization. Blindness and Vision Impairment Prevention: Priority Eye Diseases, Glaucoma. https://www.who.int/blindness/causes/priority/en/index6.html.
-
- Olthoff CMG, Schouten JSAG, van de Borne BW, Webers CAB. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112:953–961. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
