

Neuro-Ophthalmic Sarcoidosis
- PMID: 33012922
- PMCID: PMC7518323
- DOI: 10.1080/01658107.2019.1583761
Neuro-Ophthalmic Sarcoidosis
Abstract
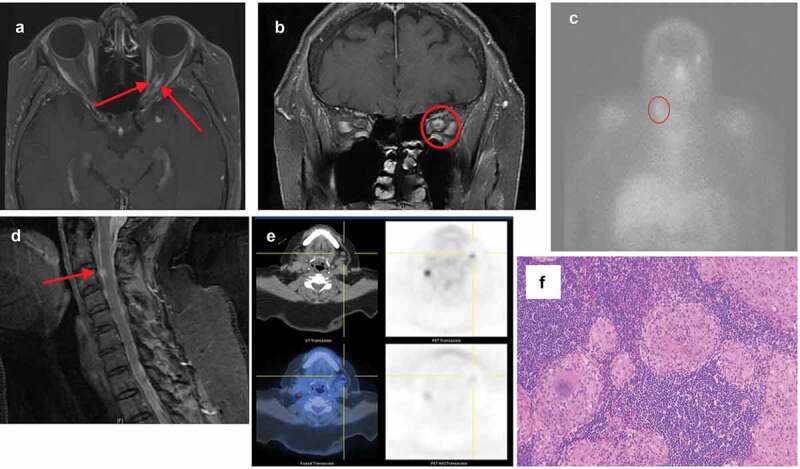
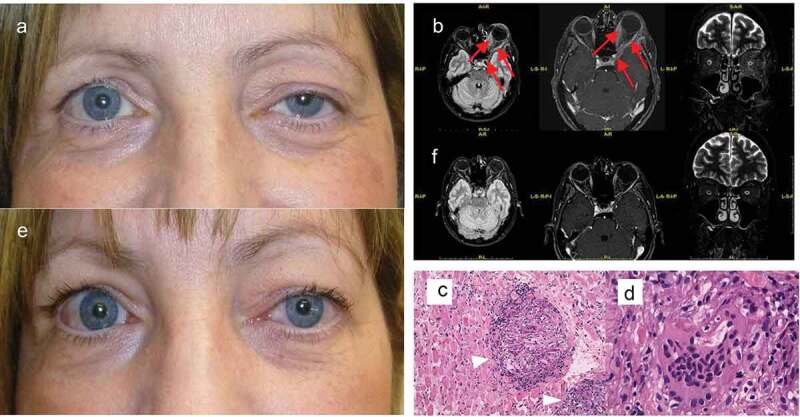
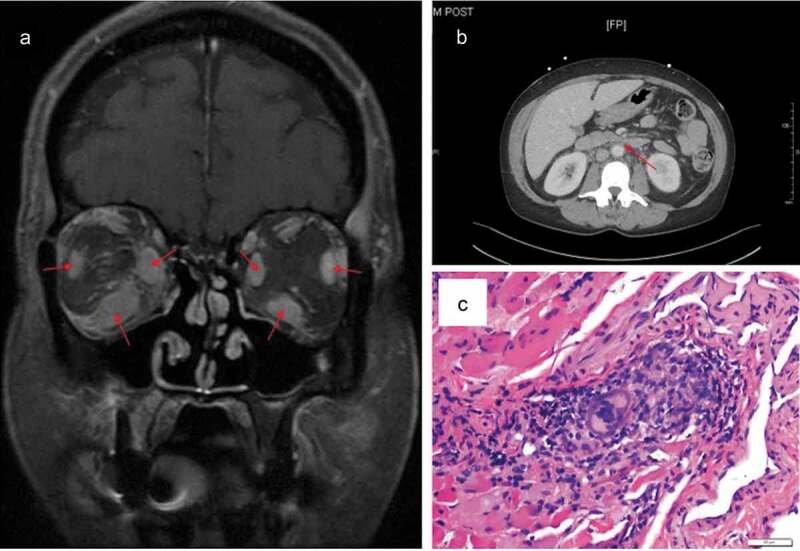
Background: In the absence of confirmatory biopsy, the criteria for diagnosis of neuro-ophthalmic sarcoidosis are not well established. Diagnostic criteria for both intraocular sarcoidosis and neurosarcoidosis have been proposed, but the diagnosis of neuro-ophthalmic sarcoidosis remains challenging. It is our intention to augment what is currently known about the diagnosis of neuro-ophthalmic sarcoidosis by providing a series of biopsy-proven cases that contribute to the continued development of diagnostic criteria for this enigmatic condition. Methods: Case series of four Caucasian women with biopsy-proven neuro-ophthalmic sarcoidosis. Results: The first patient was initially diagnosed with traumatic optic neuropathy following a fall. Years later, the presence of pathologic submandibular lymphadenopathy was identified and biopsied, revealing non-caseating granulomas. The second and third cases involved sarcoidosis of the extraocular muscles without clear or common systemic features of sarcoidosis. In the fourth and final case, the patient presented with a Horner syndrome attributed to sarcoid infiltration of the ipsilateral sympathetic chain. Bronchoscopy with biopsy showed non-caseating granulomas consistent with sarcoidosis. Conclusions: We describe four cases of neuro-ophthalmic sarcoidosis and propose possible neuro-orbital and neuro-ophthalmic criteria both with and without diagnostic biopsy.
Keywords: Neuro-ophthalmic sarcoidosis; diagnostic criteria; non-caseating granuloma; sarcoidosis.
© 2019 Taylor & Francis Group, LLC.
Figures
References
-
- Allen RKA, Stellars RE, Sandstrom PA. A prospective study of 32 patients with neurosarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2003;20:118–215. - PubMed
Publication types
LinkOut - more resources
Full Text Sources