

Effectiveness and Safety of Oral Anticoagulants in Older Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis
- PMID: 33013422
- PMCID: PMC7509201
- DOI: 10.3389/fphar.2020.583311
Effectiveness and Safety of Oral Anticoagulants in Older Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis
Abstract
Background and objective: Atrial fibrillation (AF), the most common cardiac arrhythmia, typically increases with age. Oral anticoagulants (OACs) are the cornerstone of treatment to reduce the associated risk for systemic thromboembolism. Four large randomized controlled trials (RCTs) have shown that non-vitamin K antagonist oral anticoagulants (NOACs) are non-inferior to vitamin K antagonists (VKAs) in preventing stroke and systemic embolism, as well as regarding their risk for major bleeding. However, as vulnerable geriatric patients with AF were largely underrepresented in these trials, physicians are faced with the challenge of choosing the right anticoagulant for geriatric patients in real-life clinical practice. In this vulnerable patient group, NOACs tend to be underused or underdosed due to concerns of excessive fall-related intracranial bleeding, cognitive impairment, multiple drug-drug interactions, low body weight or impaired renal function. As life expectancy continues to rise worldwide, the number of geriatric patients substantially increases. Therefore, there is an urgent need for a critical appraisal of the added value of NOACs in geriatric patients with AF at high thromboembolic and bleeding risk.
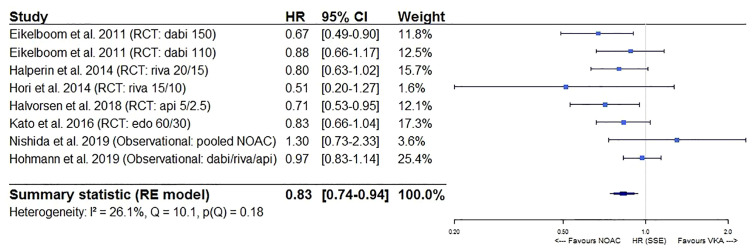
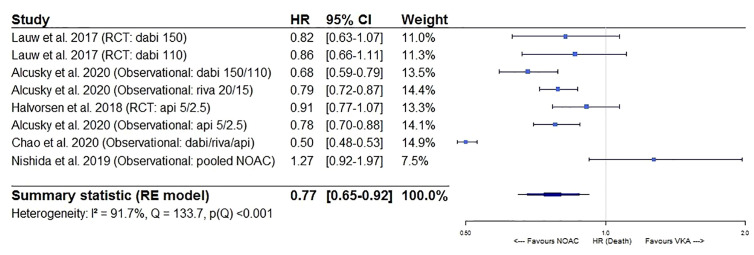
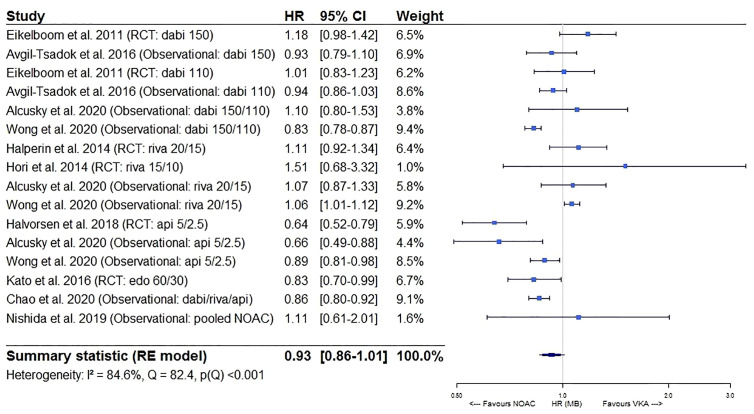
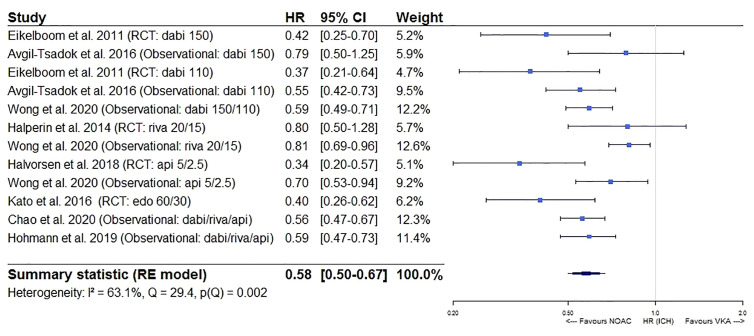
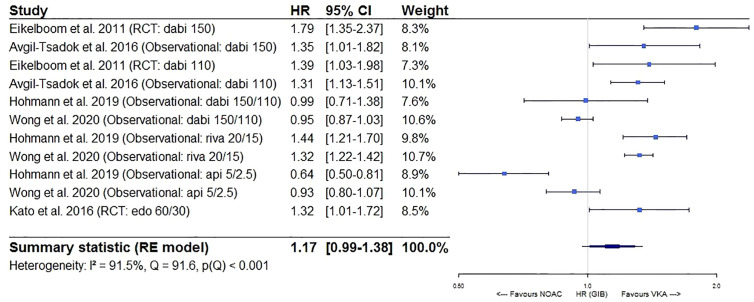
Methods and results: This systematic review provides an overview of the literature on the impact of increased age (≥75 years), multimorbidity, polypharmacy, increased falling risk, frailty and dementia on the effectiveness and safety of NOACs as compared to VKAs, after searching the Medline database. Moreover, a meta-analysis on the impact of increased age ≥75 years old was performed after pooling results from 6 post hoc analyses of RCTs and 6 longitudinal observational cohort studies, highlighting the superior effectiveness (hazard ratio (HR) 0.83, 95% confidence interval (CI) [0.74-0.94] for stroke/SE; HR 0.77, 95%CI [0.65-0.92] for mortality) and non-inferior safety (HR 0.93, 95%CI [0.86-1.01] for major bleeding; HR 0.58, 95%CI [0.50-0.67] for intracranial bleeding; HR 1.17, 95%CI [0.99-1.38] for gastrointestinal bleeding) of NOACs versus VKAs in older AF patients.
Conclusion: Across geriatric subgroups, apixaban was consistently associated with the most favourable benefit-risk profile and should therefore be preferred in geriatric patients with AF. However, research gaps on the impact of increased falling risk, frailty and baseline dementia were identified, requiring careful consideration while awaiting more results.
Keywords: atrial fibrillation; dementia; fall; frailty; increased age; multimorbidity; oral anticoagulant; polypharmacy.
Copyright © 2020 Grymonprez, Steurbaut, De Backer, Petrovic and Lahousse.
Figures
References
-
- Alcusky M., Tjia J., McManus D. D., Hume A. L., Fisher M., Lapane K. L. (2020). Comparative Safety and Effectiveness of Direct-Acting Oral Anticoagulants Versus Warfarin: a National Cohort Study of Nursing Home Residents. J. Gen. Internal Med. 35 (8), 2329–2337. 10.1007/s11606-020-05777-3 - DOI - PMC - PubMed
-
- Avin K. G., Hanke T. A., Kirk-Sanchez N., McDonough C. M., Shubert T. E., Hardage J., et al. (2015). Management of falls in community-dwelling older adults: clinical guidance statement from the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Phys. Ther. 95 (6), 815–834. 10.2522/ptj.20140415 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials