

Livedo Racemosa - The Pathophysiology of Decompression-Associated Cutis Marmorata and Right/Left Shunt
- PMID: 33013436
- PMCID: PMC7497564
- DOI: 10.3389/fphys.2020.00994
Livedo Racemosa - The Pathophysiology of Decompression-Associated Cutis Marmorata and Right/Left Shunt
Abstract
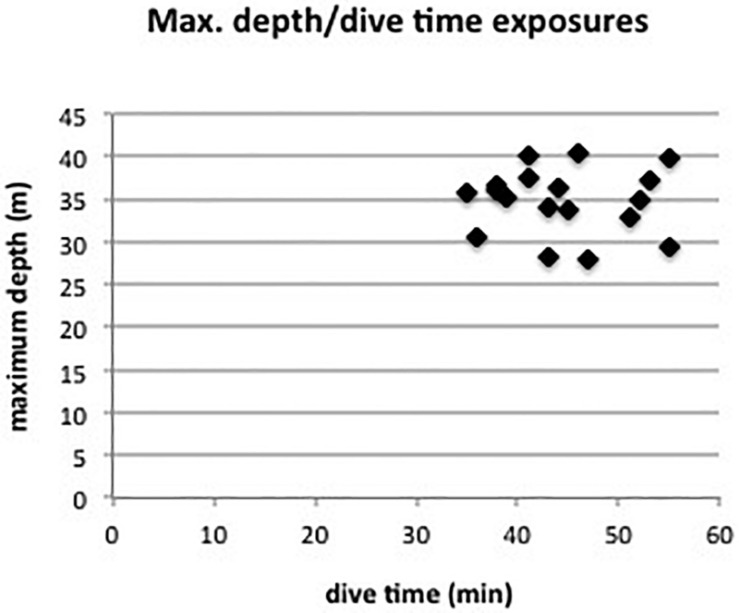
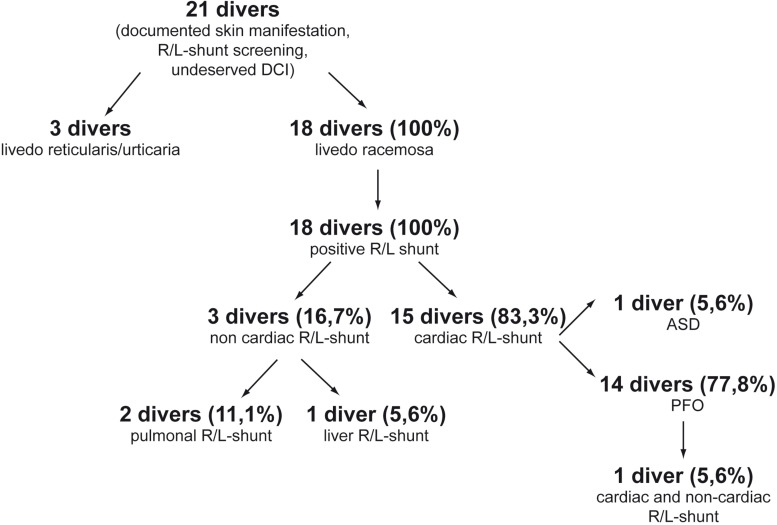
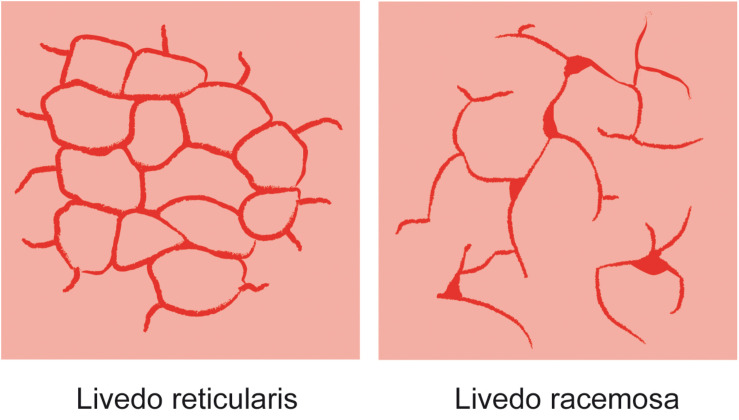
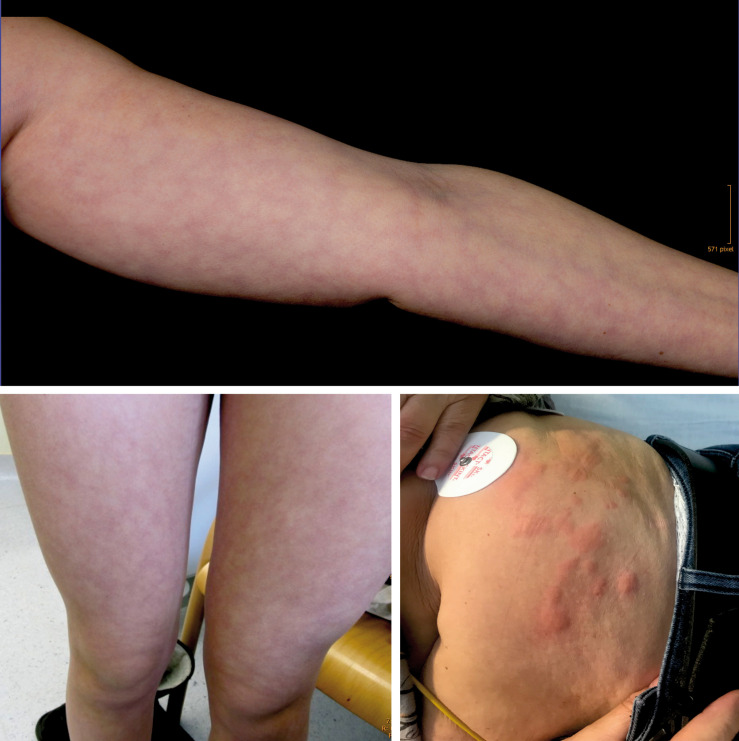
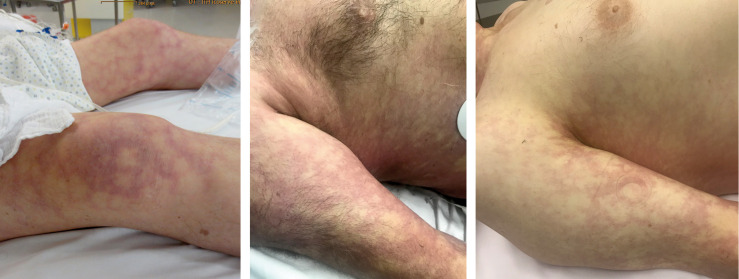
Decompression sickness and arterial gas embolism, collectively known as decompression illness (DCI), are serious medical conditions that can result from compressed gas diving. DCI can present with a wide range of physiologic and neurologic symptoms. In diving medicine, skin manifestations are usually described in general as cutis marmorata (CM). Mainly in the Anglo-American literature the terms cutis marmorata, livedo reticularis (LR), and livedo racemosa (LRC) are used interchangeably but actually describe pathophysiologically different phenomena. CM is a synonym for LR, which is a physiological and benign, livid circular discoloration with a net-like, symmetric, reversible, and uniform pattern. The decompression-associated skin discolorations, however, correspond to the pathological, irregular, broken netlike pattern of LRC. Unlike in diving medicine, in clinical medicine/dermatology the pathology of livedo racemosa is well described as a thrombotic/embolic occlusion of arteries. This concept of arterial occlusion suggests that the decompression-associated livedo racemosa may be also caused by arterial gas embolism. Recent studies have shown a high correlation of cardiac right/left (R/L) shunts with arterial gas embolism and skin bends in divers with unexplained DCI. To further investigate this hypothesis, a retrospective analysis was undertaken in a population of Austrian, Swiss, and German divers. The R/L shunt screening results of 18 divers who suffered from an unexplained decompression illness (DCI) and presented with livedo racemosa were retrospectively analyzed. All of the divers were diagnosed with a R/L shunt, 83% with a cardiac shunt [patent foramen ovale (PFO)/atrium septum defect (ASD)], and 17% with a non-cardiac shunt. We therefore not only confirm this hypothesis but when using appropriate echocardiographic techniques even found a 100% match between skin lesions and R/L shunt. In conclusion, in diving medicine the term cutis marmorata/livedo reticularis is used incorrectly for describing the actual pathology of livedo racemosa. Moreover, this pathology could be a good explanation for the high correlation of livedo racemosa with cardiac and non-cardiac right/left shunts in divers without omission of decompression procedures.
Keywords: PFO; cutis marmorata; decompression illness; livedo racemosa; livedo reticularis; patent ovale foramen; right/left shunt; skin bends.
Copyright © 2020 Hartig, Reider, Sojer, Hammer, Ploner, Muth, Tilg and Köhler.
Figures

References
-
- Balestra C., Germonpré P., Marroni A. (1998). Intrathoracic pressure changes after Valsalva strain and other maneuvers: Implications for divers with patent foramen ovale. Undersea Hyperb. Med. 25 171–174. - PubMed
-
- Buttolph T. B., Dick E. J., Toner C. B., Broome J. R., Williams R., Kang Y. H., et al. (1998). Cutaneous lesions in swine after decompression: histopathology and ultrastructure. Undersea Hyperb. Med. 25 115–121. - PubMed
LinkOut - more resources
Full Text Sources