

Bimodal Therapy for Chronic Subjective Tinnitus: A Randomized Controlled Trial of EMDR and TRT Versus CBT and TRT
- PMID: 33013517
- PMCID: PMC7511540
- DOI: 10.3389/fpsyg.2020.02048
Bimodal Therapy for Chronic Subjective Tinnitus: A Randomized Controlled Trial of EMDR and TRT Versus CBT and TRT
Abstract
Introduction: To date, guidelines recommend the use of a stepped care approach to treat tinnitus. The current clinical management of tinnitus frequently consists of audiologic interventions and tinnitus retraining therapy (TRT) or cognitive behavioral therapy (CBT). Due to the high heterogeneity of the tinnitus population and comorbidity of tinnitus with insomnia, anxiety, and depression, these interventions may not be sufficient for every patient. The current study aims to determine whether a bimodal therapy for chronic, subjective tinnitus consisting of the combination of TRT and eye movement desensitization reprocessing (EMDR) results in a clinically significant different efficacy in comparison with the prevailing bimodal TRT and CBT therapy.
Methods: Patients were randomized in two treatment groups. The experimental group received the bimodal therapy TRT/EMDR and the active control group received the bimodal therapy TRT/CBT. Evaluations took place at baseline (T0), at the end of the treatment (T1), and 3 months after therapy (T2). The tinnitus functional index (TFI) was used as primary outcome measurement. Secondary outcome measurements were the visual analog scale of tinnitus loudness (VASLoudness), tinnitus questionnaire (TQ), hospital anxiety and depression scale (HADS), hyperacusis questionnaire (HQ), global perceived effect (GPE), and psychoacoustic measurements.
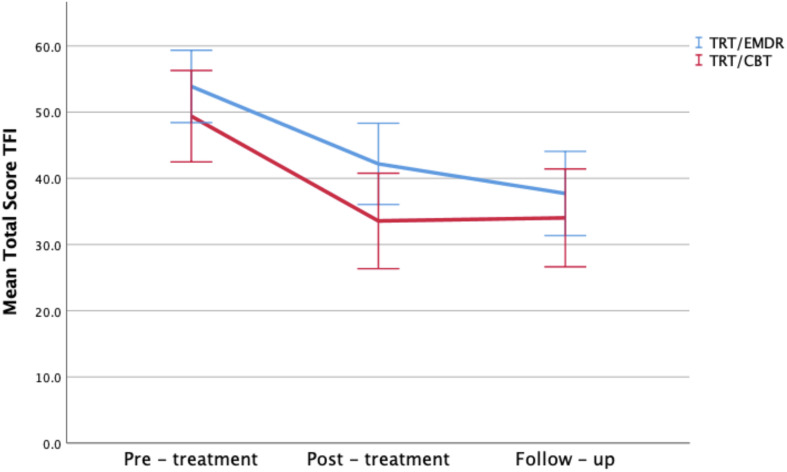
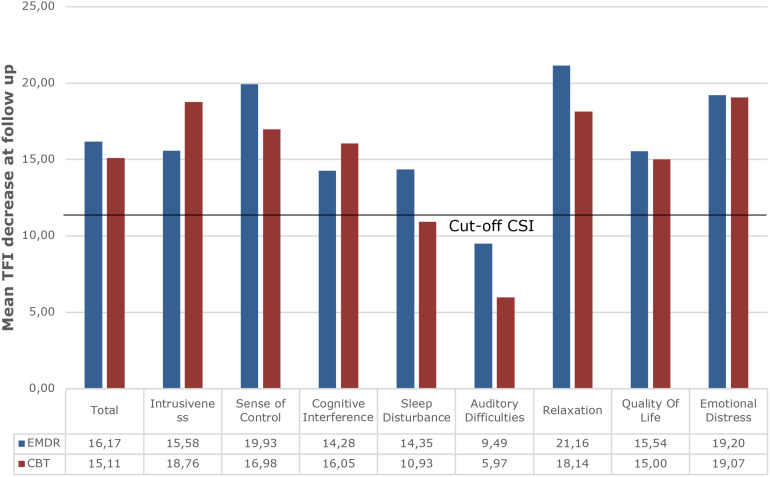
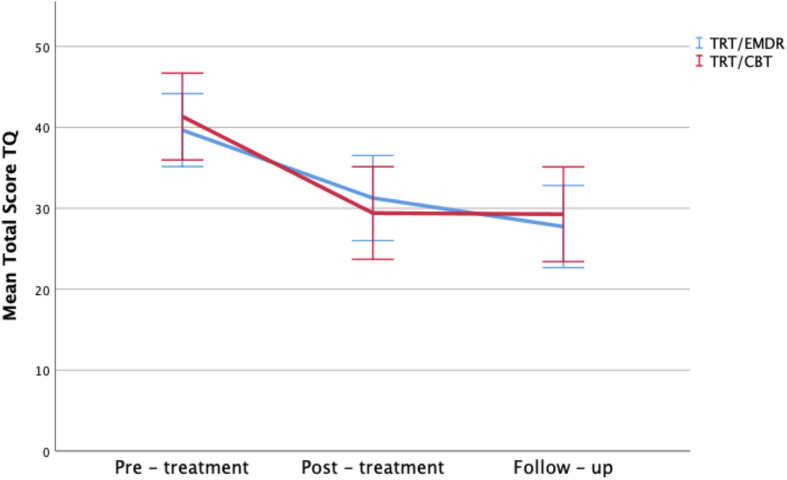
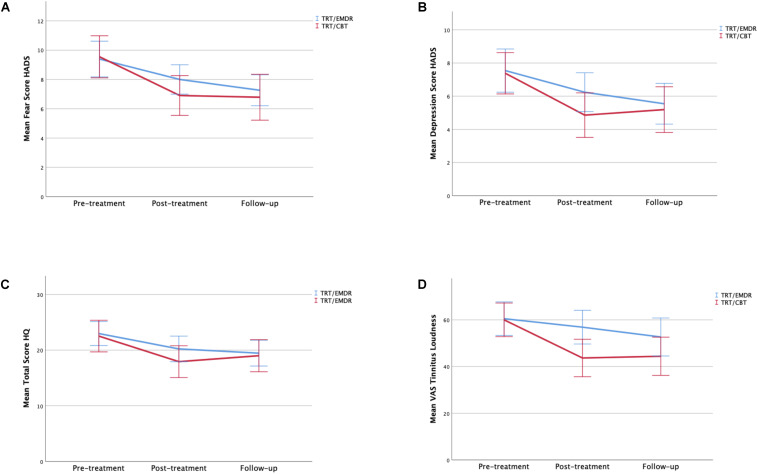
Findings: The TFI showed clinically significant improvement in both bimodal therapies (mean decrease 15.1 in TRT/CBT; p < 0.001 vs. 16.2 in TRT/EMDR; p < 0.001). The total score on the TQ, HADS, HQ, and VASLoudness all demonstrated significant decrease after treatment and follow-up (p < 0.001) in the experimental and the active control group. GPE-measurements revealed that more than 80% (i.e., 84% in TRT/CBT vs. 80% in TRT/EMDR) of the patients experienced substantial improvement of tinnitus at follow up. Treatment outcome remained stable after 3 month follow-up and no adverse events were observed.
Conclusion: Both psychotherapeutic protocols result in a clinically significant improvement for patients with chronic subjective tinnitus. No significant different efficacy was found for the TRT/EMDR treatment compared to the combination of TRT and CBT.
Clinical trial registration: ClinicalTrials.gov, ID: NCT03114878. April 14, 2017.
Keywords: bimodal therapy; chronic subjective tinnitus; cognitive behavioral therapy; eye movement desensitization and reprocessing; psychotherapy; tinnitus retraining therapy.
Copyright © 2020 Luyten, Jacquemin, Van Looveren, Declau, Fransen, Cardon, De Bodt, Topsakal, Van de Heyning, Van Rompaey and Gilles.
Figures
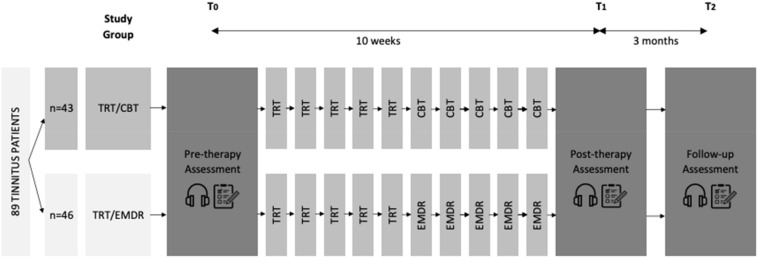
 and questionnaires
and questionnaires  were part of the assessment performed at pre-therapy (T0), post-therapy (T1), and follow-up (T2) (CBT, cognitive behavioral therapy; EMDR, eye movement desensitization and reprocessing; TRT, tinnitus retraining therapy).
were part of the assessment performed at pre-therapy (T0), post-therapy (T1), and follow-up (T2) (CBT, cognitive behavioral therapy; EMDR, eye movement desensitization and reprocessing; TRT, tinnitus retraining therapy).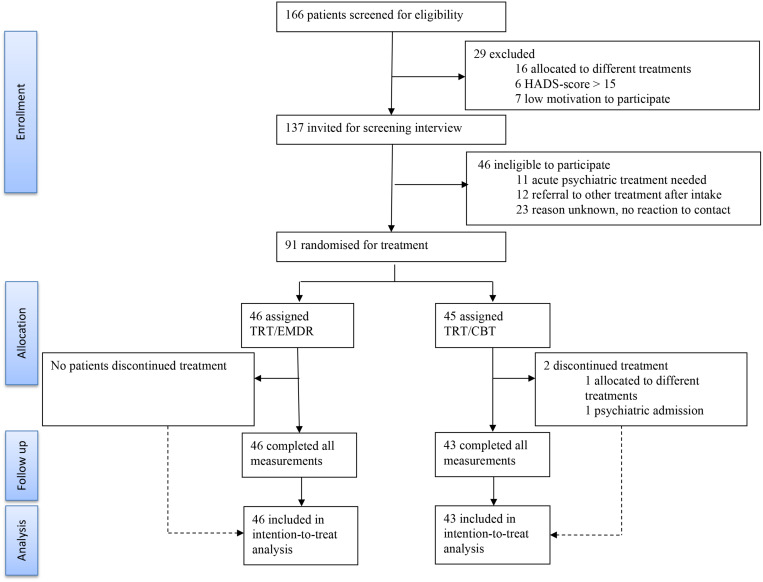
Similar articles
-
The value of Eye Movement Desensitization Reprocessing in the treatment of tinnitus: study protocol for a randomized controlled trial.Trials. 2019 Jan 9;20(1):32. doi: 10.1186/s13063-018-3121-6. Trials. 2019. PMID: 30626414 Free PMC article.
-
Sex Differences in the Response to Different Tinnitus Treatment.Front Neurosci. 2020 May 12;14:422. doi: 10.3389/fnins.2020.00422. eCollection 2020. Front Neurosci. 2020. PMID: 32477049 Free PMC article.
-
Effect of Tinnitus Retraining Therapy vs Standard of Care on Tinnitus-Related Quality of Life: A Randomized Clinical Trial.JAMA Otolaryngol Head Neck Surg. 2019 Jul 1;145(7):597-608. doi: 10.1001/jamaoto.2019.0821. JAMA Otolaryngol Head Neck Surg. 2019. PMID: 31120533 Free PMC article. Clinical Trial.
-
Cognitive behavioural therapy for tinnitus.Cochrane Database Syst Rev. 2020 Jan 8;1(1):CD012614. doi: 10.1002/14651858.CD012614.pub2. Cochrane Database Syst Rev. 2020. PMID: 31912887 Free PMC article.
-
Sound therapy (using amplification devices and/or sound generators) for tinnitus.Cochrane Database Syst Rev. 2018 Dec 27;12(12):CD013094. doi: 10.1002/14651858.CD013094.pub2. Cochrane Database Syst Rev. 2018. PMID: 30589445 Free PMC article.
Cited by
-
Current and Emerging Therapies for Chronic Subjective Tinnitus.J Clin Med. 2023 Oct 16;12(20):6555. doi: 10.3390/jcm12206555. J Clin Med. 2023. PMID: 37892692 Free PMC article. Review.
-
Eye Movement Desensitization and Reprocessing (EMDR) treatment in the medical setting: a systematic review.Eur J Psychotraumatol. 2024;15(1):2341577. doi: 10.1080/20008066.2024.2341577. Epub 2024 May 15. Eur J Psychotraumatol. 2024. PMID: 38747113 Free PMC article.
-
Cost-effectiveness of a smartphone Application for Tinnitus Treatment (the CATT trial): a study protocol of a randomised controlled trial.Trials. 2022 May 23;23(1):435. doi: 10.1186/s13063-022-06378-7. Trials. 2022. PMID: 35606823 Free PMC article.
-
When the Mind Meets the Ear: A Scoping Review on Tinnitus and Clinically Measured Psychiatric Comorbidities.J Clin Med. 2025 May 28;14(11):3785. doi: 10.3390/jcm14113785. J Clin Med. 2025. PMID: 40507547 Free PMC article. Review.
References
-
- Baguley D., McFerran D., Hall D. (2013). Tinnitus. Lancet 382 1600–1607. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous