

Dryness of Foot Skin Assessed by the Visual Indicator Test and Risk of Diabetic Foot Ulceration: A Prospective Observational Study
- PMID: 33013702
- PMCID: PMC7506164
- DOI: 10.3389/fendo.2020.00625
Dryness of Foot Skin Assessed by the Visual Indicator Test and Risk of Diabetic Foot Ulceration: A Prospective Observational Study
Abstract
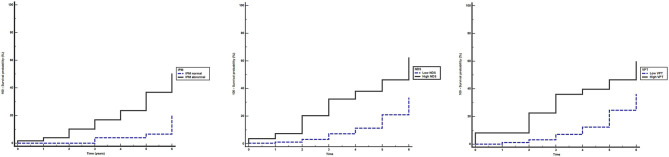
Research Question: Previous cross-sectional studies have shown an association between sudomotor dysfunction and diabetic foot ulceration (DFU). The aim of this prospective multicenter study was to determine the role of dryness of foot skin and of established neurological modalities in the prediction of risk for foot ulceration in a cohort of individuals with diabetes mellitus (DM). Design: The study was conducted from 2012 to 2017. A total of 308 subjects with DM without history of DFU or critical limb ischemia completed the study. Diabetic neuropathy was assessed using the neuropathy symptom score (NSS) and neuropathy disability score (NDS). In a subset of participants, vibration perception threshold (VPT) was evaluated. Dryness of foot skin was assessed by the visual indicator plaster method (IPM). The diagnostic performance of the above neurological modalities for prediction of DFU was tested by receiver operating characteristic curve (ROC) analysis. Results: During the 6-year follow-up, 55 patients (annual ulceration incidence 2.97%) developed DFU. Multivariate Cox-regression analysis after controlling for the effect of age, gender, and DM duration demonstrated that the risk (hazard ratio, 95% confidence intervals) of DFU increased significantly with either abnormal IPM (3.319, 1.460-7.545, p = 0.004) or high (≥6) NDS (2.782, 1.546-5.007, p = 0.001) or high (≥25 volts) VPT (2.587, 1.277-5.242, p = 0.008). ROC analysis showed that all neurological modalities could discriminate participants who developed DFU (p < 0.001). IPM testing showed high sensitivity (0.86) and low specificity (0.49), while high vs. low NDS and VPT showed low sensitivity (0.40 and 0.39, respectively) and high specificity (0.87 and 0.89, respectively) for identification of patients at risk for DFU. Conclusion: Dryness of foot skin assessed by the IPM predicts the development of DFU. IPM testing has high sensitivity, whereas high NDS and VPT have high specificity in identifying subjects at risk for DFU. The IPM can be included in the screening methods for identification of the foot at risk.
Keywords: diabetes; foot ulcer; indicator plaster method; neuropad; neuropathy disability score; risk; vibration perception.
Copyright © 2020 Panagoulias, Eleftheriadou, Papanas, Manes, Kamenov, Tesic, Bousboulas, Tentolouris, Jude and Tentolouris.
Figures
References
-
- Prompers L, Huijberts M, Apelqvist J, Jude E, Piaggesi A, Bakker K, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. (2007) 50:18–25. 10.1007/s00125-006-0491-1 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical