

Association Between Galactose-Deficient IgA1 Derived From the Tonsils and Recurrence of IgA Nephropathy in Patients Who Underwent Kidney Transplantation
- PMID: 33013875
- PMCID: PMC7494805
- DOI: 10.3389/fimmu.2020.02068
Association Between Galactose-Deficient IgA1 Derived From the Tonsils and Recurrence of IgA Nephropathy in Patients Who Underwent Kidney Transplantation
Abstract
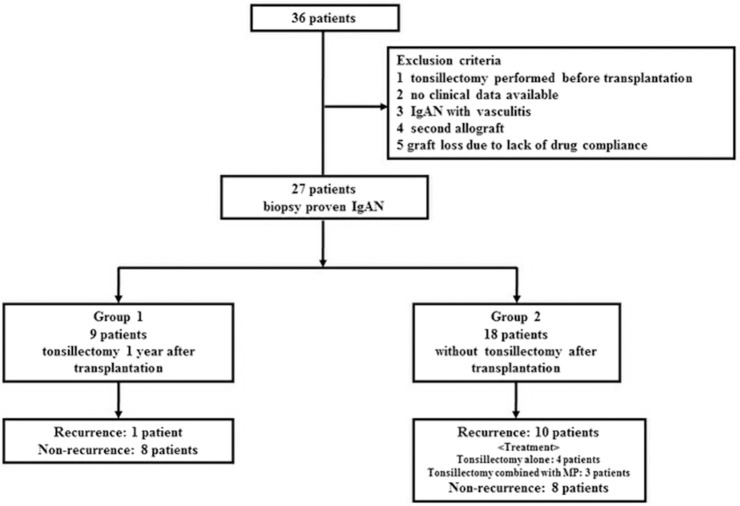
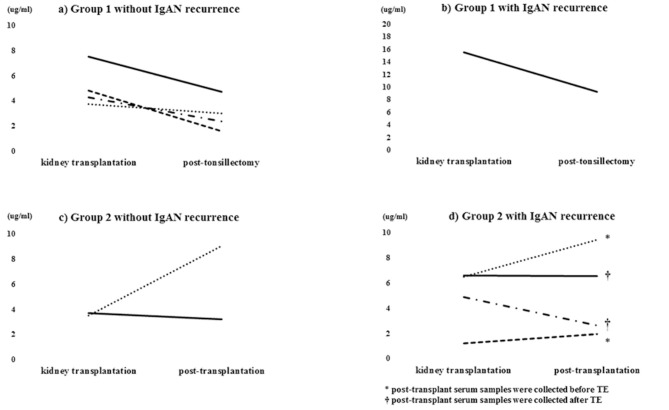
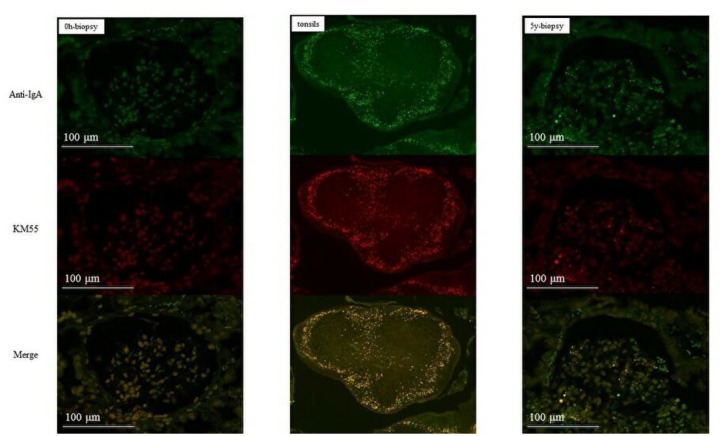
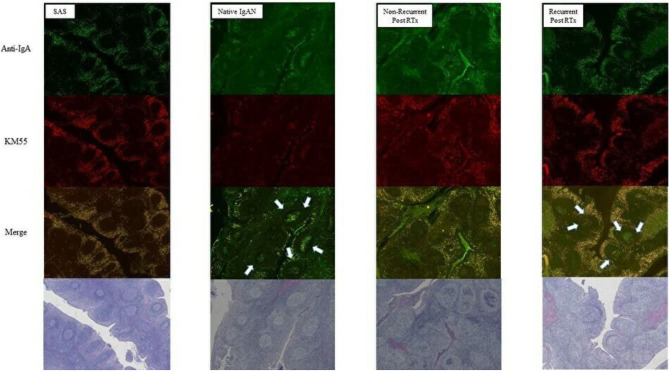
Background: Recurrence of IgA nephropathy (IgAN) in the transplanted kidney is associated with graft survival, but no specific treatment is available. Tonsillectomy (TE) reportedly arrests the progression of IgAN in the native kidney. Thus, we conducted a single-center retrospective cohort study to evaluate the effect of TE prior to IgAN recurrence. Methods: Of the 36 patients with biopsy-proven IgAN who underwent kidney transplantation, 27 were included in this study. Nine patients underwent TE at 1 year after kidney transplantation (group 1), and the remaining 18 did not undergo TE (group 2). Results: The rate of histological IgAN recurrence was significantly lower in group 1 than in group 2 (11.1 vs. 55.6%, log-rank p = 0.046). In addition, half of the recurrent patients in group 2 exhibited active lesions, compared to none in group 1. Serum Gd-IgA1 levels decreased after TE in group 1, whereas they remained stable or increased slightly in group 2. In the recurrent cases, IgA and Gd-IgA1 were found in the germinal center in addition to the mantle zone of tonsils. Finally, mesangial IgA and Gd-IgA1 immunoreactivity was reduced after TE in some cases. Conclusion: Our data suggest that TE at 1 year after kidney transplantation might be associated with the reduced rate of histological IgAN recurrence. TE arrested or reduced serum Gd-IgA1 and mesangial Gd-IgA1 immunoreactivity. Therefore, we generated a hypothesis that serum Gd-IgA1 derived from the tonsils may play a pivotal role in the pathogenesis of IgAN. Based on these findings, we need to conduct verification in a prospective randomized controlled trial.
Keywords: IgA nephropathy; galactose-deficient IgA1; kidney transplantation; recurrent glomerulonephritis; tonsillectomy.
Copyright © 2020 Kawabe, Yamamoto, Yamakawa, Katsumata, Isaka, Katsuma, Nakada, Kobayashi, Koike, Ueda, Tanno, Koike, Miki, Yamada, Kimura, Ohkido, Tsuboi, Yamamoto, Kojima and Yokoo.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous