

Pericardial effusion with tamponade - an uncommon presentation leading to the diagnosis of eosinophilic granulomatosis polyangiitis: A case report
- PMID: 33014293
- PMCID: PMC7509990
- DOI: 10.4330/wjc.v12.i9.460
Pericardial effusion with tamponade - an uncommon presentation leading to the diagnosis of eosinophilic granulomatosis polyangiitis: A case report
Abstract
Background: Eosinophilic granulomatosis polyangiitis (EGPA) is a small vessel necrotizing vasculitis that commonly presents as peripheral eosinophilia and asthma; however, it can rarely manifest with cardiac involvement such as pericarditis and cardiac tamponade. Isolated pericardial tamponade presenting as the initial symptom of EGPA is exceedingly rare. Early diagnosis and appropriate treatment are crucial to prevent life-threatening outcomes.
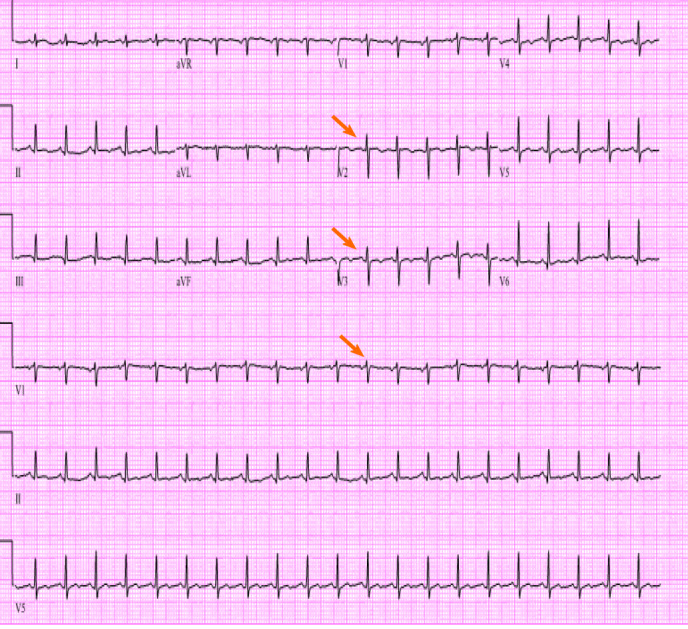
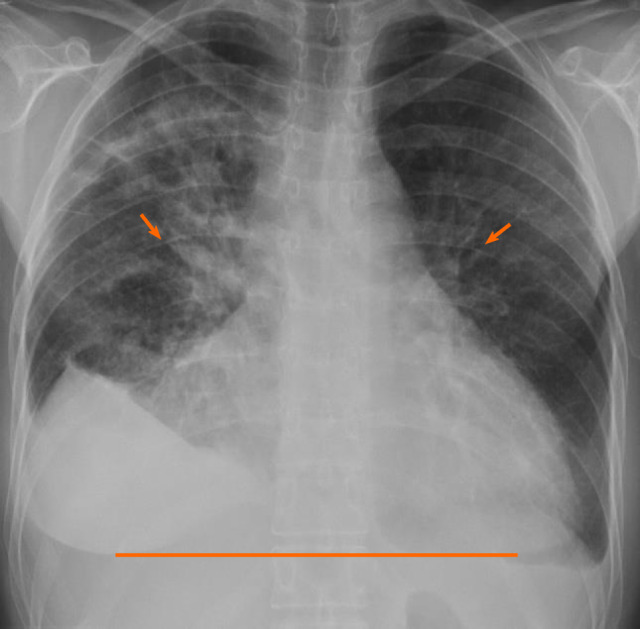
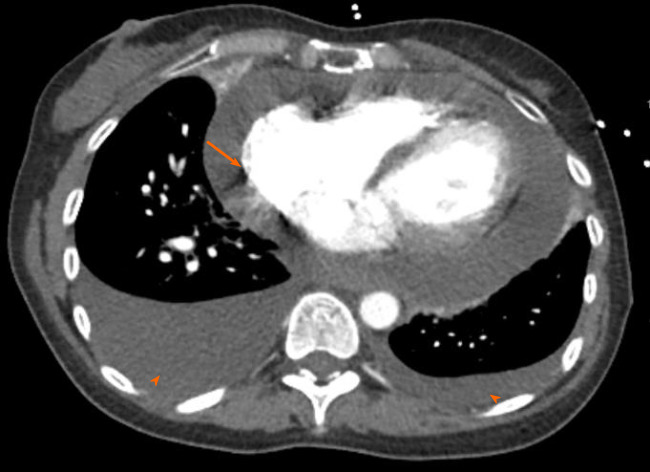
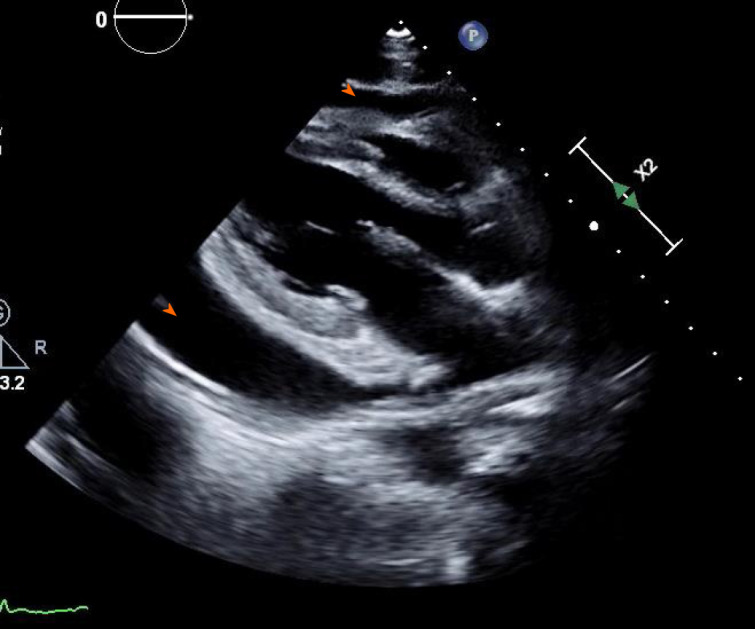
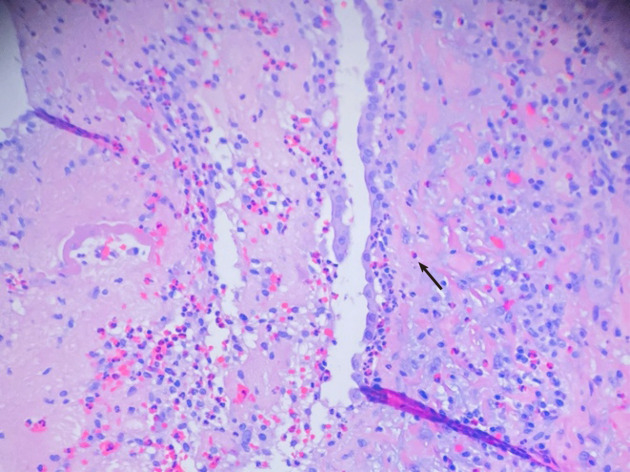
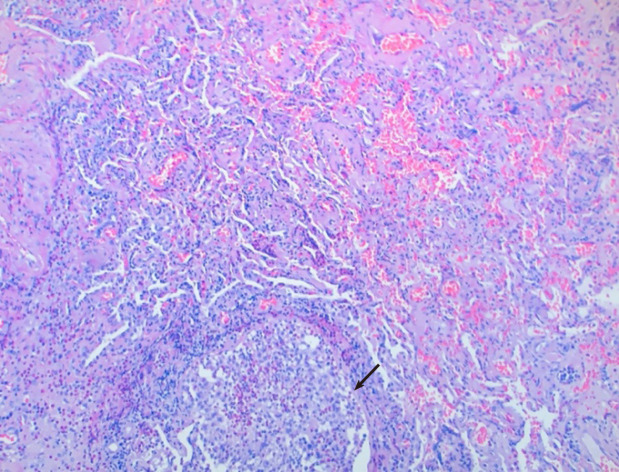
Case summary: 52-year-old woman with no past medical history presented with progressive dyspnea and dry cough. On physical exam she had a pericardial friction rub and bilateral rales. Vital signs were notable for tachycardia at 119 beats per minute and hypoxia with 89% oxygen saturation. On laboratory exam, she had 45% peripheral eosinophilia, troponin elevation of 1.1 ng/mL and N-terminal prohormone of brain natriuretic peptide of 2101 pg/mL. TTE confirmed a large pericardial effusion and tamponade physiology. She underwent urgent pericardial window procedure. Pericardial and lung biopsy demonstrated eosinophilic infiltration. Based on the American College of Radiology guidelines, the patient was diagnosed with EGPA which manifested in its rare form of cardiac tamponade. She was treated with steroid taper and mepolizumab.
Conclusion: This case highlights that when isolated pericardial involvement occurs in EGPA, diagnosis is recognized by performing pericardial biopsy demonstrating histopathologic evidence of eosinophilic infiltration.
Keywords: Cardiac tamponade; Case report; Eosinophilic granulomatosis polyangiitis; Mepolizumab; Pericardial biopsy; Pericardial effusion; Peripheral eosinophilia.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no potential financial interests.
Figures
References
-
- Watts RA, Lane S, Scott DG. What is known about the epidemiology of the vasculitides? Best Pract Res Clin Rheumatol. 2005;19:191–207. - PubMed
-
- Agard C, Rendu E, Leguern V, Ponge T, Masseau A, Barrier JH, Trochu JN, Hamidou MA, Guillevin L. Churg-Strauss syndrome revealed by granulomatous acute pericarditis: two case reports and a review of the literature. Semin Arthritis Rheum. 2007;36:386–391. - PubMed
-
- Yano T, Ishimura S, Furukawa T, Koyama M, Tanaka M, Shimoshige S, Hashimoto A, Miura T. Cardiac tamponade leading to the diagnosis of eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome): a case report and review of the literature. Heart Vessels. 2015;30:841–844. - PubMed
-
- Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis) Arthritis Rheum. 1990;33:1094–1100. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
