

Geographic and socioeconomic considerations for glioblastoma treatment in the elderly at a national level: a US perspective
- PMID: 33014393
- PMCID: PMC7516121
- DOI: 10.1093/nop/npaa029
Geographic and socioeconomic considerations for glioblastoma treatment in the elderly at a national level: a US perspective
Abstract
Background: Treatment for glioblastoma (GBM) in elderly (age > 65 years) patients can be affected by multiple geographic and socioeconomic parameters. Correspondingly, the aim of this study was to determine trends in treatment of elderly GBM patients in the United States.
Methods: All GBM patients in the U.S. National Cancer Database between 2005 and 2016 were retrospectively reviewed. Status of treatment by triple therapy (resection, chemotherapy, and radiation) were summarized and analyzed by U.S. Census region.
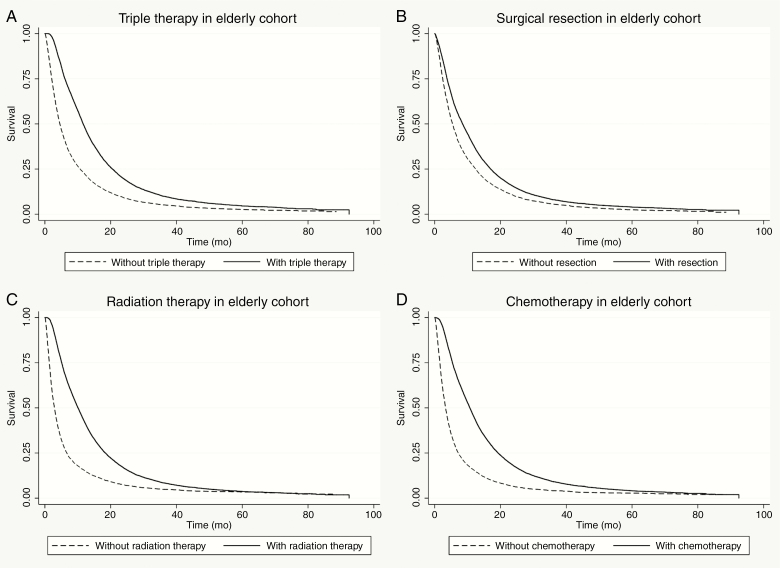
Results: There were 44 338 GBM patients included, with 21 573 (49%) elderly and 22 765 (51%) nonelderly patients with median ages 72 years (range, 65-90 years) and 47 years (range, 40-64 years), respectively. Compared to nonelderly patients, elderly patients had significantly lower odds of being treated by triple therapy (odds ratio, OR = 0.54) as a whole, and its individual elements of resection (OR = 0.78), chemotherapy (OR = 0.46), radiation therapy (OR = 0.52). This was reflected in each U.S. Census region, with the lowest odds of being treated with triple therapy, surgical resection, chemotherapy, and radiation therapy in New England (OR = 0.51) Mountain (OR = 0.66), West North Central (OR = 0.38), and the Middle Atlantic (OR = 0.44), respectively. Multivariable analysis revealed multiple socioeconomic parameters that significantly predicted lower odds of triple therapy in the elderly.
Conclusions: In the United States alone, there exists geographic disparity in the treatment outcomes of elderly GBM patients. Multiple socioeconomic parameters can influence access to treatment modalities for elderly patients compared to younger patients in different geographic regions, and public health initiatives targeting these aspects may prove beneficial conceptually to optimize and homogenize clinical outcomes.
Keywords: access; disparity; elderly; geographic; glioblastoma.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

Similar articles
-
Geographic disparities in access to glioblastoma treatment based on Hispanic ethnicity in the United States: Insights from a national database.J Neurooncol. 2020 May;147(3):711-720. doi: 10.1007/s11060-020-03480-1. Epub 2020 Mar 31. J Neurooncol. 2020. PMID: 32236779
-
Combined-Modality Therapy With Radiation and Chemotherapy for Elderly Patients With Glioblastoma in the Temozolomide Era: A National Cancer Database Analysis.JAMA Neurol. 2016 Jul 1;73(7):821-8. doi: 10.1001/jamaneurol.2016.0839. JAMA Neurol. 2016. PMID: 27214765
-
Outcomes and Patterns of Care in Elderly Patients with Glioblastoma Multiforme.World Neurosurg. 2021 May;149:e1026-e1037. doi: 10.1016/j.wneu.2021.01.028. Epub 2021 Jan 20. World Neurosurg. 2021. PMID: 33482415
-
The role of radiation therapy in treatment of adults with newly diagnosed glioblastoma multiforme: a systematic review and evidence-based clinical practice guideline update.J Neurooncol. 2020 Nov;150(2):215-267. doi: 10.1007/s11060-020-03612-7. Epub 2020 Nov 19. J Neurooncol. 2020. PMID: 33215344
-
Management of glioblastoma in elderly patients.J Neurol Sci. 2017 Sep 15;380:250-255. doi: 10.1016/j.jns.2017.07.048. Epub 2017 Aug 1. J Neurol Sci. 2017. PMID: 28870580 Free PMC article. Review.
Cited by
-
Disparities in Reported Testing for 1p/19q Codeletion in Oligodendroglioma and Oligoastrocytoma Patients: An Analysis of the National Cancer Database.Front Oncol. 2021 Nov 9;11:746844. doi: 10.3389/fonc.2021.746844. eCollection 2021. Front Oncol. 2021. PMID: 34858822 Free PMC article.
-
Newly Diagnosed Glioblastoma in Elderly Patients.Curr Oncol Rep. 2022 Mar;24(3):325-334. doi: 10.1007/s11912-022-01201-7. Epub 2022 Feb 5. Curr Oncol Rep. 2022. PMID: 35122621 Free PMC article. Review.
-
Optimal managements of elderly patients with glioblastoma.Jpn J Clin Oncol. 2022 Aug 5;52(8):833-842. doi: 10.1093/jjco/hyac075. Jpn J Clin Oncol. 2022. PMID: 35552425 Free PMC article. Review.
-
Area-level socioeconomic status is positively correlated with glioblastoma incidence and prognosis in the United States.Front Oncol. 2023 Mar 17;13:1110473. doi: 10.3389/fonc.2023.1110473. eCollection 2023. Front Oncol. 2023. PMID: 37007113 Free PMC article. Review.
-
Lack of survival advantage among re-resected elderly glioblastoma patients: a SEER-Medicare study.Neurooncol Adv. 2020 Nov 29;3(1):vdaa159. doi: 10.1093/noajnl/vdaa159. eCollection 2021 Jan-Dec. Neurooncol Adv. 2020. PMID: 33506202 Free PMC article.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Cohen-Inbar O. Geriatric brain tumor management part II: glioblastoma multiforme. J Clin Neurosci. 2019;67:1–4. - PubMed
-
- Lorimer CF, Saran F, Chalmers AJ, Brock J.. Glioblastoma in the elderly—how do we choose who to treat? J Geriatr Oncol. 2016;7(6):453–456. - PubMed
-
- Lerro CC, Robbins AS, Phillips JL, Stewart AK.. Comparison of cases captured in the National Cancer Data Base with those in population-based central cancer registries. Ann Surg Oncol. 2013;20(6):1759–1765. - PubMed
