

Case Series of Perforated Keratomycosis after Laser-Assisted In Situ Keratomileusis
- PMID: 33014490
- PMCID: PMC7512097
- DOI: 10.1155/2020/7237903
Case Series of Perforated Keratomycosis after Laser-Assisted In Situ Keratomileusis
Abstract
Background: Fungal keratitis is an extremely rare complication of laser vision correction resulting in poor visual outcomes. Amniotic membrane transplantation should be kept in mind in eyes with corneal perforation prior to penetrating keratoplasty.
Aim: To assess the outcomes of multilayered fresh amniotic membrane transplantation (MLF-AMT) in patients with severe keratomycosis after laser-assisted in situ keratomileusis (LASIK). Study design. Hospital-based prospective interventional case series.
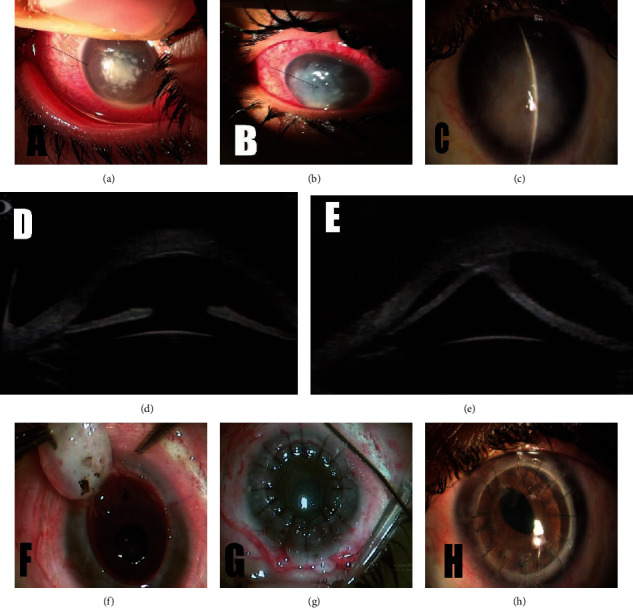
Methods: Five eyes of 5 patients were included in the study. All cases underwent microbiological scrapings from residual bed and intrastromal injections of amphotericin (50 mcg/mL), with flap amputation if needed, followed by topical 5% natamycin and 0.15% amphotericin. MLF-AMT was performed after corneal perforation. Later, penetrating keratoplasty (PK) was performed when corneal opacity compromised visual acuity. The outcome measures were complete resolution of infection, corneal graft survival, and best-corrected visual acuity (BCVA).
Results: The mean age of patients was 22 ± 1.2 years with 4/5 (80%) were females. The mean interval between LASIK and symptom onset was 8.8 ± 1 day, and the mean interval between symptom onset and referral was 14 ± 1.4 days. Potassium hydroxide (KOH) smears showed filamentous fungi, and Sabouraud's medium grew Aspergillus in all cases. Melted flaps were amputated in 4 (80%) cases. MLF-AMT was performed in all cases due to corneal perforation after a mean time of 12.4 ± 1.2 days of antifungals. In all cases, complete resolution of infection was seen 26 ± 1.8 days after MLF-AMT, and optical PK was done at a mean of 2.4 months later. No postoperative complications after MLF-AMT or PK were observed, with a 0% incidence of corneal graft rejection, and a final BCVA ranged from 20/20 to 20/80 after a mean follow-up of 14 ± 1.1 months.
Conclusion: MLF-AMT is a safe and valid option to manage corneal perforation during keratmycosis treatment to avoid emergency therapeutic keratoplasty.
Copyright © 2020 Taher Eleiwa et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
Post-laser in situ keratomileusis interface fungal keratitis.Cornea. 2014 Oct;33(10):1022-30. doi: 10.1097/ICO.0000000000000227. Cornea. 2014. PMID: 25170582
-
Long-term comparison of full-bed deep lamellar keratoplasty with penetrating keratoplasty in treating corneal leucoma caused by herpes simplex keratitis.Am J Ophthalmol. 2012 Feb;153(2):291-299.e2. doi: 10.1016/j.ajo.2011.07.020. Epub 2011 Oct 13. Am J Ophthalmol. 2012. PMID: 21996306
-
Surgical outcomes of perforated and unperforated corneal descemetocele.Int Ophthalmol. 2018 Feb;38(1):327-335. doi: 10.1007/s10792-017-0472-z. Epub 2017 Feb 21. Int Ophthalmol. 2018. PMID: 28224301
-
[Partial visual rehabilitation 5 and 6 years after a Gundersen total conjunctival flap procedure].Ophthalmologe. 2022 Feb;119(2):203-208. doi: 10.1007/s00347-021-01503-4. Epub 2021 Sep 28. Ophthalmologe. 2022. PMID: 34581853 Review. German.
-
Infectious interface keratitis (IIK) following lamellar keratoplasty: A literature review.Ocul Surf. 2019 Oct;17(4):635-643. doi: 10.1016/j.jtos.2019.08.001. Epub 2019 Aug 12. Ocul Surf. 2019. PMID: 31415815
Cited by
-
Recent Advances in Diagnosis and Treatment Approaches in Fungal Keratitis: A Narrative Review.Microorganisms. 2024 Jan 13;12(1):161. doi: 10.3390/microorganisms12010161. Microorganisms. 2024. PMID: 38257986 Free PMC article. Review.
-
Debulking corneal biopsy with tectonic amniotic membrane transplantation in refractory clinically presumed fungal keratitis.Sci Rep. 2024 Jan 4;14(1):521. doi: 10.1038/s41598-023-50987-4. Sci Rep. 2024. PMID: 38177182 Free PMC article.
-
Amniotic membrane transplantation in a 2-month-old infant with toxic epidermal necrolysis.Am J Ophthalmol Case Rep. 2021 Jan 15;21:101017. doi: 10.1016/j.ajoc.2021.101017. eCollection 2021 Mar. Am J Ophthalmol Case Rep. 2021. PMID: 33521381 Free PMC article.
-
Recent Perspectives in the Management of Fungal Keratitis.J Fungi (Basel). 2021 Oct 26;7(11):907. doi: 10.3390/jof7110907. J Fungi (Basel). 2021. PMID: 34829196 Free PMC article. Review.
-
Amniotic membrane transplantation for infectious keratitis: a systematic review and meta-analysis.Sci Rep. 2021 Jun 21;11(1):13007. doi: 10.1038/s41598-021-92366-x. Sci Rep. 2021. PMID: 34155280 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
