

Influence of Frailty on Outcome in Older Patients Undergoing Non-Cardiac Surgery - A Systematic Review and Meta-Analysis
- PMID: 33014537
- PMCID: PMC7505262
- DOI: 10.14336/AD.2019.1024
Influence of Frailty on Outcome in Older Patients Undergoing Non-Cardiac Surgery - A Systematic Review and Meta-Analysis
Abstract
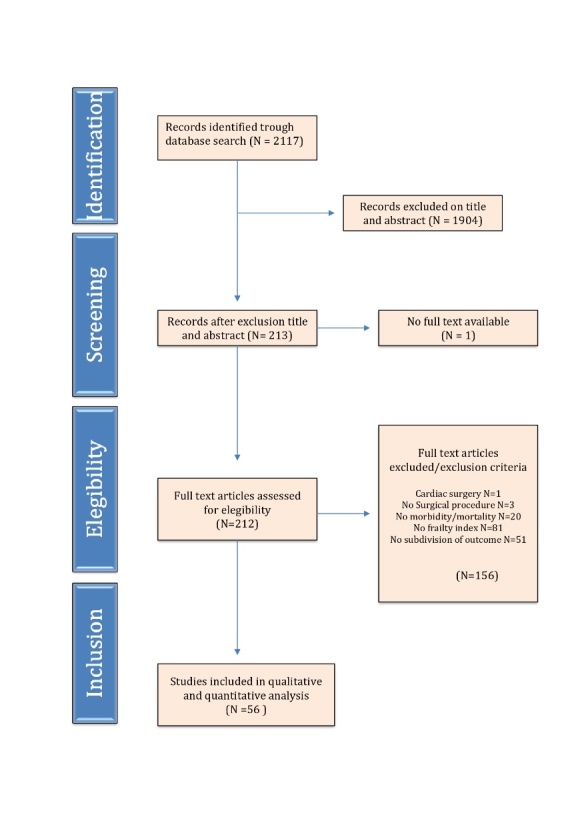
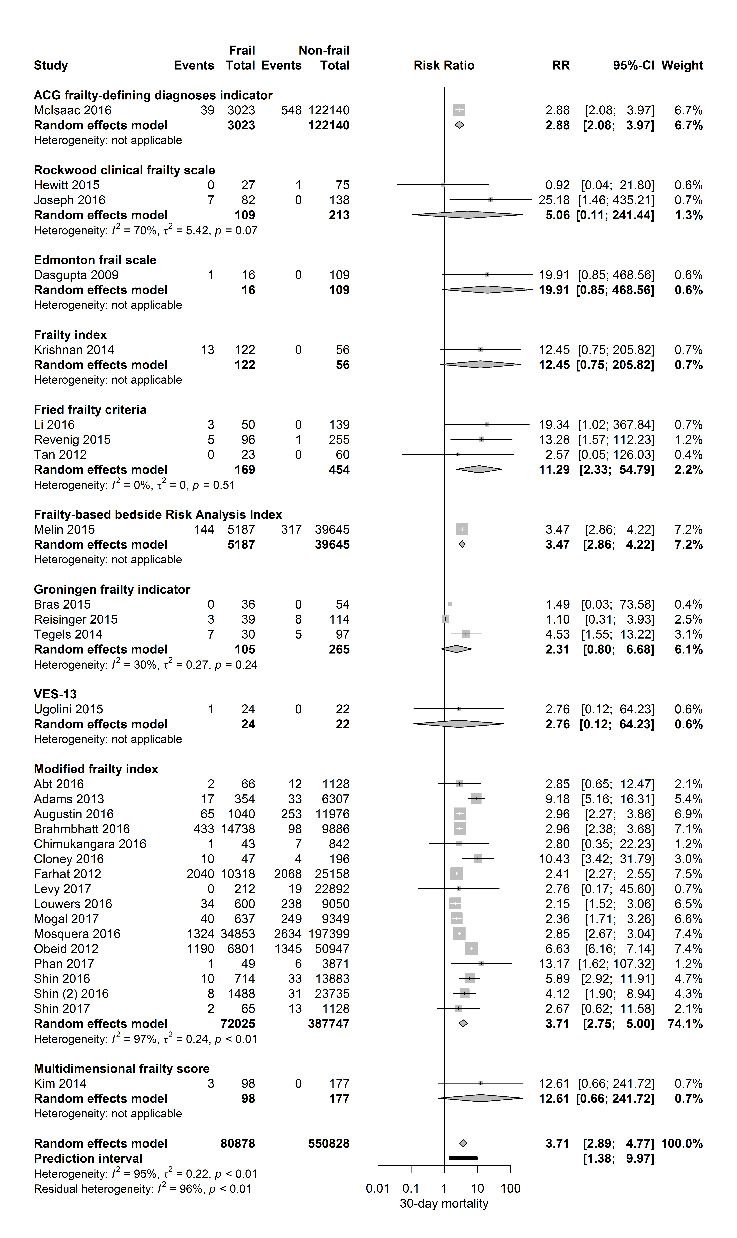
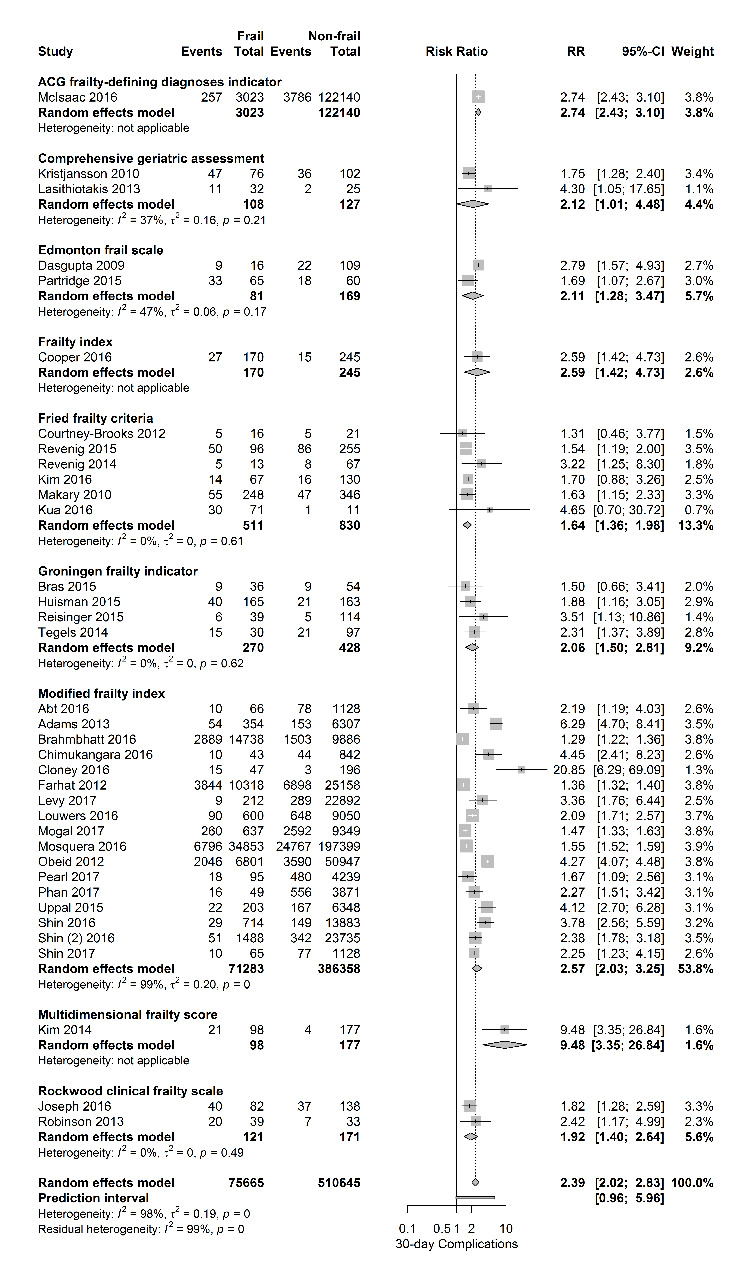
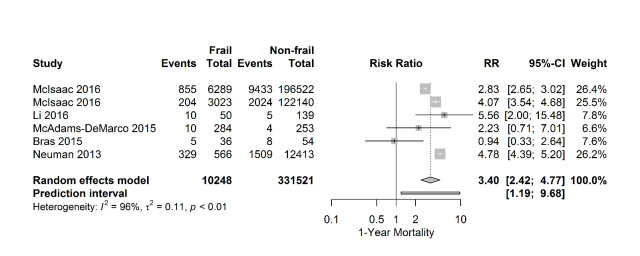
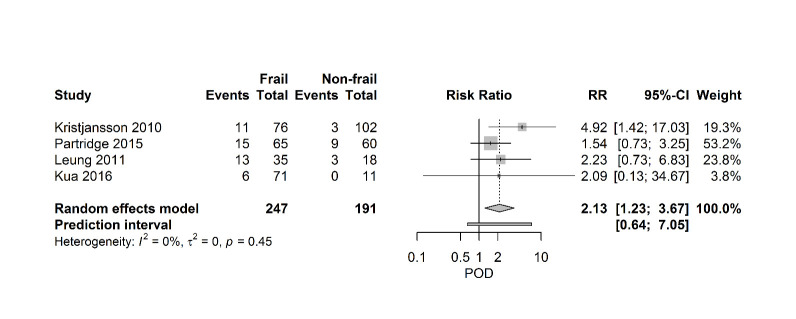
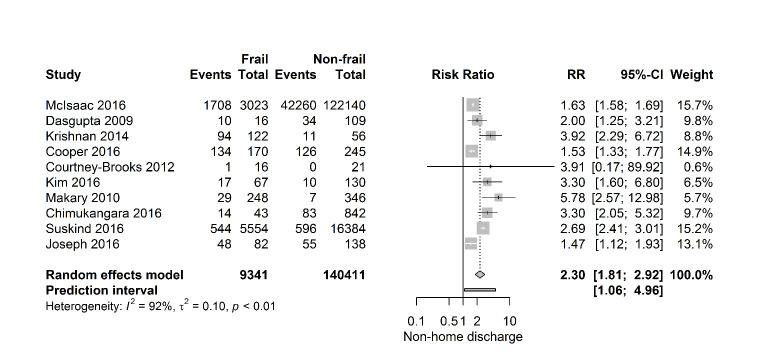
Frailty is increasingly recognized as a better predictor of adverse postoperative events than chronological age. The objective of this review was to systematically evaluate the effect of frailty on postoperative morbidity and mortality. Studies were included if patients underwent non-cardiac surgery and if frailty was measured by a validated instrument using physical, cognitive and functional domains. A systematic search was performed using EMBASE, MEDLINE, Web of Science, CENTRAL and PubMed from 1990 - 2017. Methodological quality was assessed using an assessment tool for prognosis studies. Outcomes were 30-day mortality and complications, one-year mortality, postoperative delirium and discharge location. Meta-analyses using random effect models were performed and presented as pooled risk ratios with confidence intervals and prediction intervals. We included 56 studies involving 1.106.653 patients. Eleven frailty assessment tools were used. Frailty increases risk of 30-day mortality (31 studies, 673.387 patients, risk ratio 3.71 [95% CI 2.89-4.77] (PI 1.38-9.97; I2=95%) and 30-day complications (37 studies, 627.991 patients, RR 2.39 [95% CI 2.02-2.83). Risk of 1-year mortality was threefold higher (six studies, 341.769 patients, RR 3.40 [95% CI 2.42-4.77]). Four studies (N=438) reported on postoperative delirium. Meta-analysis showed a significant increased risk (RR 2.13 [95% CI 1.23-3.67). Finally, frail patients had a higher risk of institutionalization (10 studies, RR 2.30 [95% CI 1.81- 2.92]). Frailty is strongly associated with risk of postoperative complications, delirium, institutionalization and mortality. Preoperative assessment of frailty can be used as a tool for patients and doctors to decide who benefits from surgery and who doesn't.
Keywords: frailty; non-cardiac surgery; older patients; outcome; surgery.
copyright: © 2020 Tjeertes et al.
Figures
References
-
- Mangano DT (2004). Perioperative medicine: NHLBI working group deliberations and recommendations. J Cardiothorac Vasc Anesth, 18:1-6. - PubMed
-
- Partridge JS, Harari D, Dhesi JK (2012). Frailty in the older surgical patient: a review. Age Ageing, 41:142-147. - PubMed
-
- Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, De Hert S, et al. (2014). 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur J Anaesthesiol, 31:517-573. - PubMed
-
- Lee DH, Buth KJ, Martin BJ, Yip AM, Hirsch GM (2010). Frail patients are at increased risk for mortality and prolonged institutional care after cardiac surgery. Circulation, 121:973-978. - PubMed
-
- Polanczyk CA, Marcantonio E, Goldman L, Rohde LE, Orav J, Mangione CM, et al. (2001). Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med, 134:637-643. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous