

Prospective detection of cervical dysplasia with scanning angle-resolved low coherence interferometry
- PMID: 33014608
- PMCID: PMC7510862
- DOI: 10.1364/BOE.401000
Prospective detection of cervical dysplasia with scanning angle-resolved low coherence interferometry
Abstract
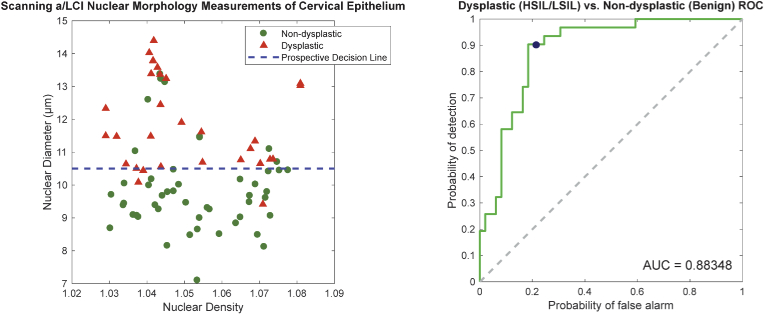
We present a prospective clinical study using angle-resolved low-coherence interferometry (a/LCI) to detect cervical dysplasia via depth resolved nuclear morphology measurements. The study, performed at the Jacobi Medical Center, compares 80 a/LCI optical biopsies taken from 20 women with histopathological tissue diagnosis of co-registered physical biopsies. A novel instrument was used for this study that enables 2D scanning across the cervix without repositioning the probe. The main study goal was to compare performance with a previous clinical a/LCI point-probe instrument [Int. J. Cancer140, 1447 (2017)] and use the same diagnostic criteria as in that study. Tissue was classified in two schemes: non-dysplastic vs. dysplastic and low-risk vs. high-risk, with the latter classification aligned with clinically actionable diagnosis. High sensitivity (non-dysplastic vs. dysplastic: 0.903, low-risk vs. high-risk: 1.000) and NPV (0.930 and 1.000 respectively) were obtained when using the previously established decision boundaries, showing the success of the scanning a/LCI instrument and reinforcing the clinical viability of a/LCI in disease detection.
© 2020 Optical Society of America under the terms of the OSA Open Access Publishing Agreement.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures











References
-
- Cuzick J., Clavel C., Petry K., M. Meijer C. J. L., Hoyer H., Ratnam S., Szarewski A., Birembaut P., Kulasingam S., Sasieni P., Iftner T., “Overview of the european and north american studies on hpv testing in primary cervical cancer screening,” Int. J. Cancer 119(5), 1095–1101 (2006). 10.1002/ijc.21955 - DOI - PubMed
-
- Yu B., Ferris D. G., Liu Y., Nagarajan V. K., “Emerging optical techniques for detection of oral, cervical and anal cancer in low-resource settings,” Austin J. Biomed. Eng. 1(2), 1007 (2014).
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources