

Incidence, Prognostic Factors and Survival for Hemangioblastoma of the Central Nervous System: Analysis Based on the Surveillance, Epidemiology, and End Results Database
- PMID: 33014882
- PMCID: PMC7509109
- DOI: 10.3389/fonc.2020.570103
Incidence, Prognostic Factors and Survival for Hemangioblastoma of the Central Nervous System: Analysis Based on the Surveillance, Epidemiology, and End Results Database
Abstract
Background: Hemangioblastomas are uncommon, benign neoplasms of the central nervous system (CNS). This study aims to evaluate the incidence, demographics, clinical characteristics, and prognosis of CNS hemangioblastomas using the data from the Surveillance, Epidemiology, and End Results (SEER) Program.
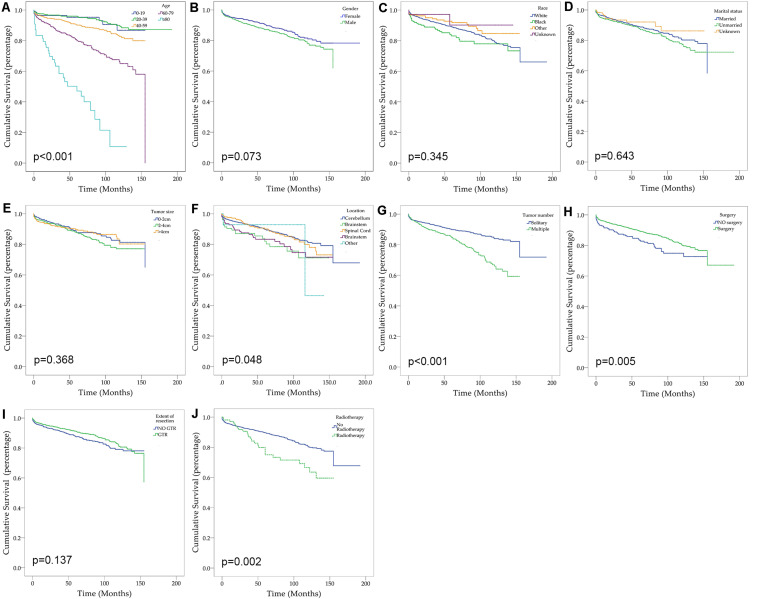
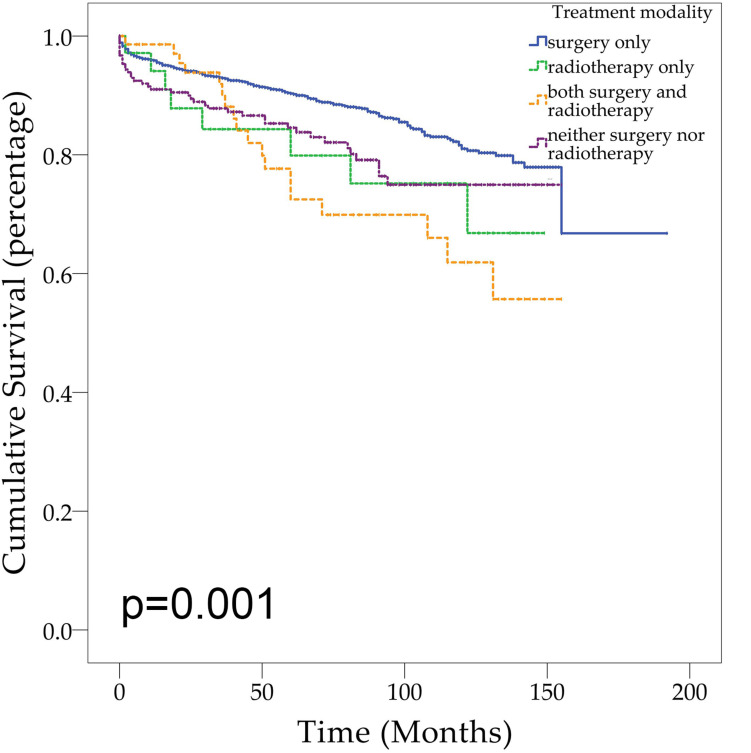
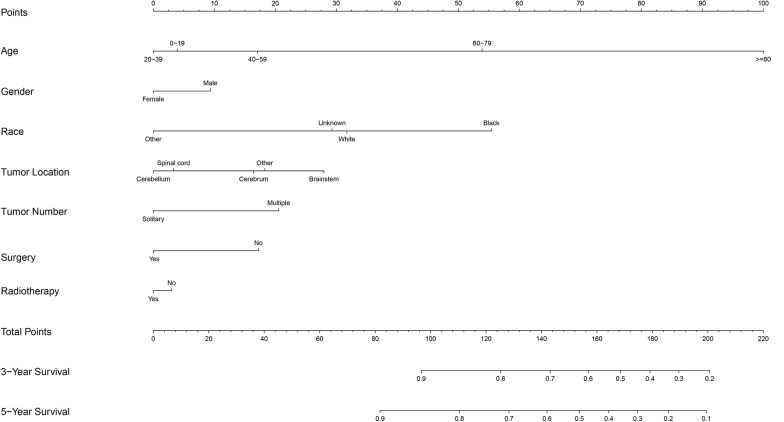
Methods: Univariate and multivariate analyses using the Cox proportional hazards model were employed to identify prognostic factors of overall survival. The Kaplan-Meier method was utilized to evaluate overall survival distribution by treatment modality. A nomogram was further built to predict survival at 3 and 5 years.
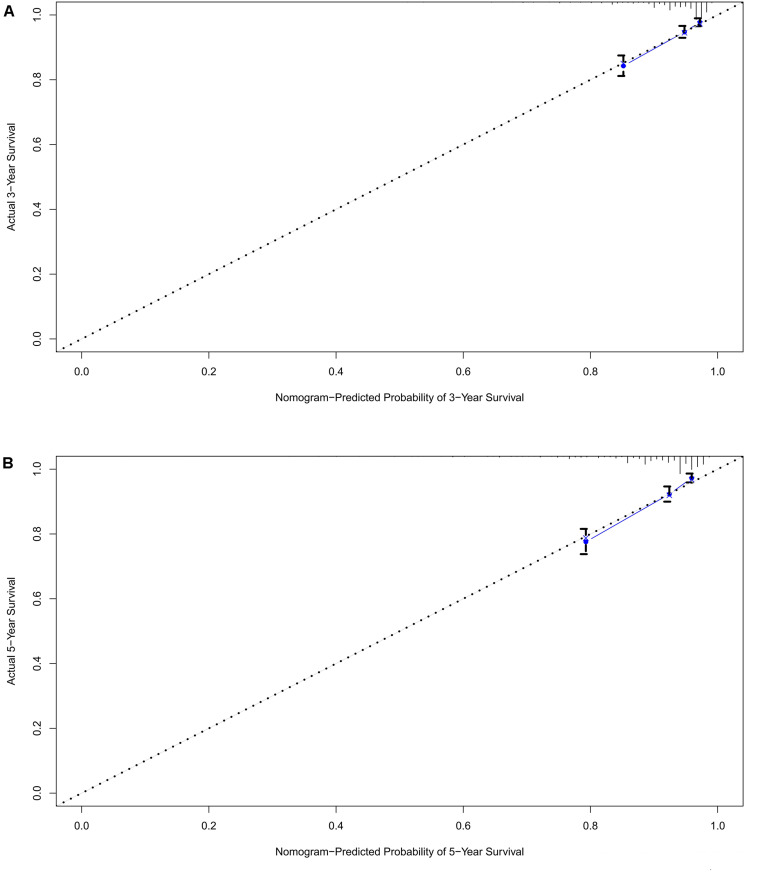
Results: The overall incidence rate of CNS hemangioblastomas was 0.141 per 100,000 person-years. Through univariate analysis and multivariate analyses, age between 60 and 79 years (HR = 3.697, p < 0.001), age greater than 80 years (HR = 12.318, p < 0.001), African American race (HR = 1.857, p = 0.003), multiple tumors (HR = 1.715, p < 0.001), and prior surgery (HR = 0.638, p = 0.013) were significantly associated with overall survival. Patients receiving surgery alone had better overall survival compared with patients receiving no treatment (p = 0.008) and patients receiving both surgery and radiotherapy (p = 0.002). The calibration plots demonstrated an excellent agreement between nomogram-predicted and actual survival.
Conclusion: In conclusion, age, race, tumor location, number of tumors, and prior surgery are prognostic factors for survival. Surgery was the most common modality and was suggested as an effective and optimal treatment. The proposed nomogram can predict the prognosis of patients with CNS hemangioblastomas and help clinicians in making decisions.
Keywords: SEER; hemangioblastoma; incidence; nomogram; prognosis; survival; treatment.
Copyright © 2020 Yin, Duan, Yi, Li, Lu and Li.
Figures
References
LinkOut - more resources
Full Text Sources