

Telemedicine as the New Outpatient Clinic Gone Digital: Position Paper From the Pandemic Health System REsilience PROGRAM (REPROGRAM) International Consortium (Part 2)
- PMID: 33014958
- PMCID: PMC7505101
- DOI: 10.3389/fpubh.2020.00410
Telemedicine as the New Outpatient Clinic Gone Digital: Position Paper From the Pandemic Health System REsilience PROGRAM (REPROGRAM) International Consortium (Part 2)
Abstract
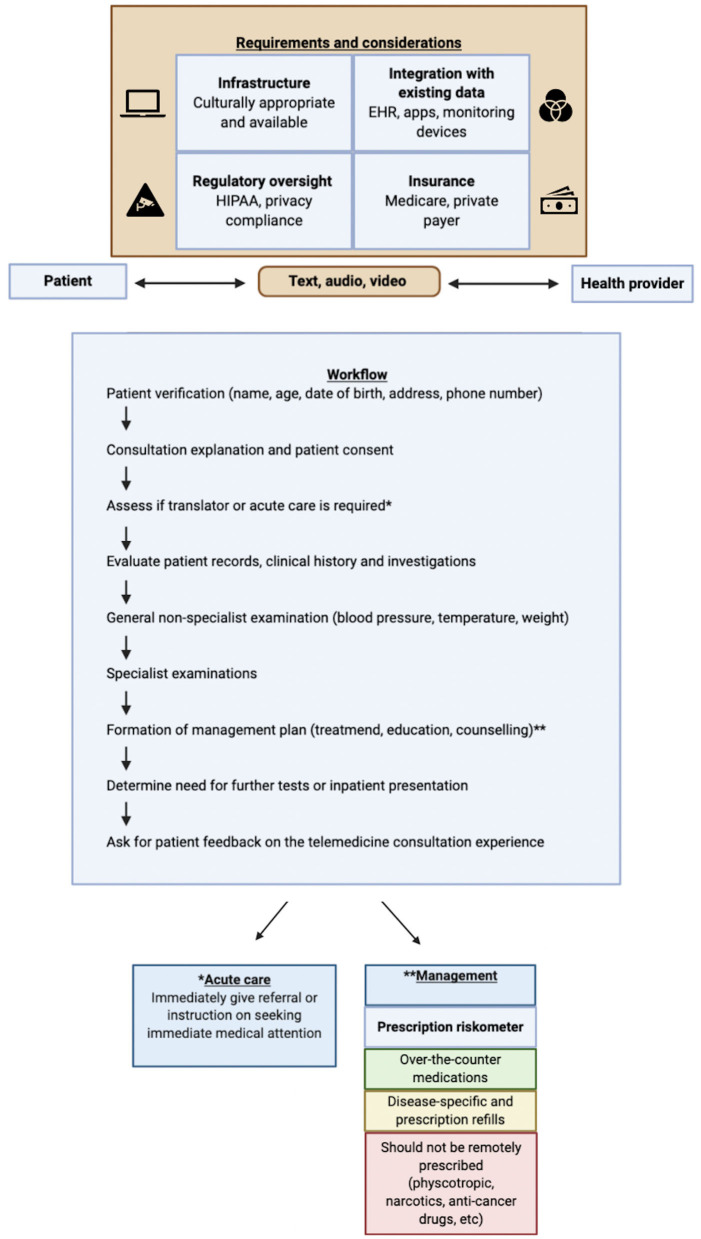
Technology has acted as a great enabler of patient continuity through remote consultation, ongoing monitoring, and patient education using telephone and videoconferencing in the coronavirus disease 2019 (COVID-19) era. The devastating impact of COVID-19 is bound to prevail beyond its current reign. The vulnerable sections of our community, including the elderly, those from lower socioeconomic backgrounds, those with multiple comorbidities, and immunocompromised patients, endure a relatively higher burden of a pandemic such as COVID-19. The rapid adoption of different technologies across countries, driven by the need to provide continued medical care in the era of social distancing, has catalyzed the penetration of telemedicine. Limiting the exposure of patients, healthcare workers, and systems is critical in controlling the viral spread. Telemedicine offers an opportunity to improve health systems delivery, access, and efficiency. This article critically examines the current telemedicine landscape and challenges in its adoption, toward remote/tele-delivery of care, across various medical specialties. The current consortium provides a roadmap and/or framework, along with recommendations, for telemedicine uptake and implementation in clinical practice during and beyond COVID-19.
Keywords: COVID-19; coronavirus disease 2019; telemedicine; teleneurology; telepsychiatry; telerehabilitation.
Copyright © 2020 Bhaskar, Bradley, Chattu, Adisesh, Nurtazina, Kyrykbayeva, Sakhamuri, Moguilner, Pandya, Schroeder, Banach and Ray.
Figures
References
-
- Bhaskar S, Rastogi A, Chattu VK, Adisesh A, Thomas P, Alvarado N, et al. Key Strategies for clinical management and improvement of healthcare services for cardiovascular disease and diabetes patients in the coronavirus (COVID-19) settings: recommendations from the REPROGRAM consortium. Front Cardiovasc Med. (2020) 7:112. 10.3389/fcvm.2020.00112 - DOI - PMC - PubMed
-
- American Telemedicine Association About Telemedicine. Available online at: http://legacy.americantelemed.org/main/about/about-telemedicine/telemedi... (accessed April 16, 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical