

Current clinical methods of measurement of respiratory rate give imprecise values
- PMID: 33015146
- PMCID: PMC7520170
- DOI: 10.1183/23120541.00023-2020
Current clinical methods of measurement of respiratory rate give imprecise values
Abstract
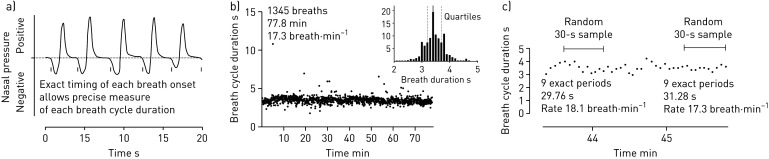
Background: Respiratory rate is a basic clinical measurement used for illness assessment. Errors in measuring respiratory rate are attributed to observer and equipment problems. Previous studies commonly report rate differences ranging from 2 to 6 breaths·min-1 between observers.
Methods: To study why repeated observations should vary so much, we conducted a virtual experiment, using continuous recordings of breathing from acutely ill patients. These records allowed each breathing cycle to be precisely timed. We made repeated random measures of respiratory rate using different sample durations of 30, 60 and 120 s. We express the variation in these repeated rate measurements for the different sample durations as the interquartile range of the values obtained for each subject. We predicted what values would be found if a single measure, taken from any patient, were repeated and inspected boundary values of 12, 20 or 25 breaths·min-1, used by the UK National Early Warning Score, for possible mis-scoring.
Results: When the sample duration was nominally 30 s, the mean interquartile range of repeated estimates was 3.4 breaths·min-1. For the 60 s samples, the mean interquartile range was 3 breaths·min-1, and for the 120 s samples it was 2.5 breaths·min-1. Thus, repeat clinical counts of respiratory rate often differ by >3 breaths·min-1. For 30 s samples, up to 40% of National Early Warning Scores could be misclassified.
Conclusions: Early warning scores will be unreliable when short sample durations are used to measure respiratory rate. Precision improves with longer sample duration, but this may be impractical unless better measurement methods are used.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: G.B. Drummond reports a grant from the Edinburgh and Lothians Health Foundation for a previous study, not this one. Conflict of interest: D. Fischer has nothing to disclose. Conflict of interest: D.K. Arvind reports grants from the Edinburgh and Lothians Health Foundation during the conduct of the study, and patents on a “Method, Apparatus, Computer Program and System for Measuring Oscillatory Motion” issued in China (number ZL 2011 8 0027571.9, November 2015) and the USA (number US 9724019, August 2017).
Figures



References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous