

Morphological Features of the Ulnar Collateral Ligament of the Elbow and Common Tendon of Flexor-Pronator Muscles
- PMID: 33015213
- PMCID: PMC7509733
- DOI: 10.1177/2325967120952415
Morphological Features of the Ulnar Collateral Ligament of the Elbow and Common Tendon of Flexor-Pronator Muscles
Abstract
Background: The anterior bundle (AB) of the ulnar collateral ligament is the most important structure for valgus stabilization of the elbow. However, anatomic relationships among the AB, posterior bundle (PB) of the ulnar collateral ligament, and common tendon (CT) of the flexor-pronator muscles have not been fully clarified.
Purpose: To classify the AB, PB, and CT and to clarify their morphological features.
Study design: Descriptive laboratory study.
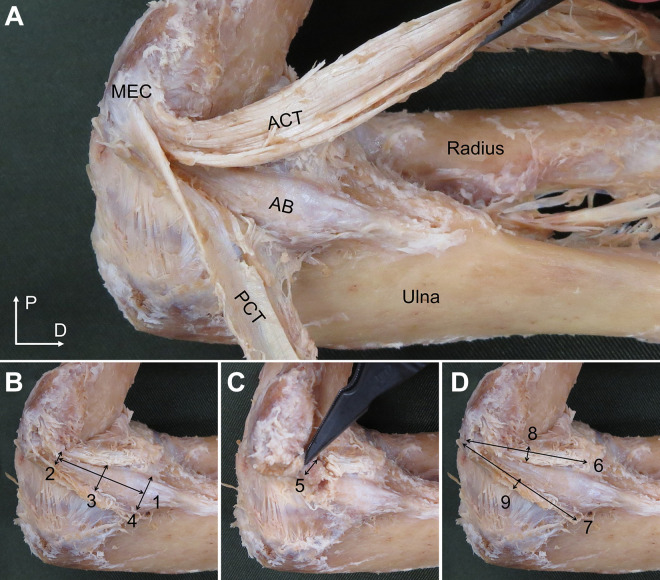
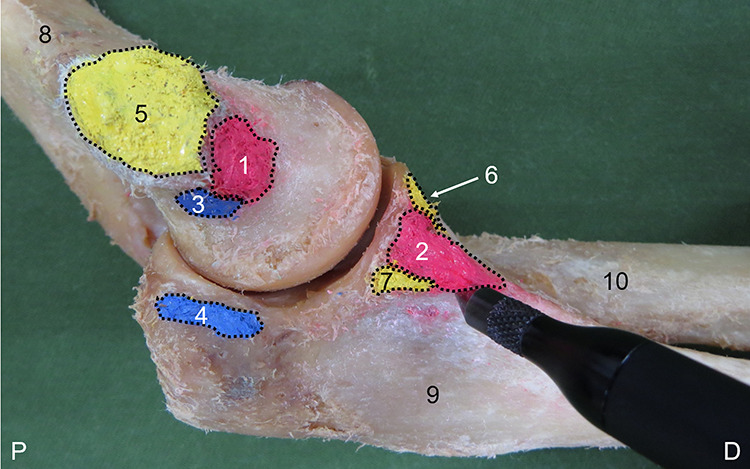
Methods: This investigation examined 56 arms from 31 embalmed Japanese cadavers. The CT investigation examined 34 arms from 23 embalmed Japanese cadavers with CTs remaining. Type classification was performed by focusing on positional relationships with surrounding structures. Morphological features measured were length, width, thickness, and footprint for the AB and PB and attachment length, thickness, and footprint for the CT.
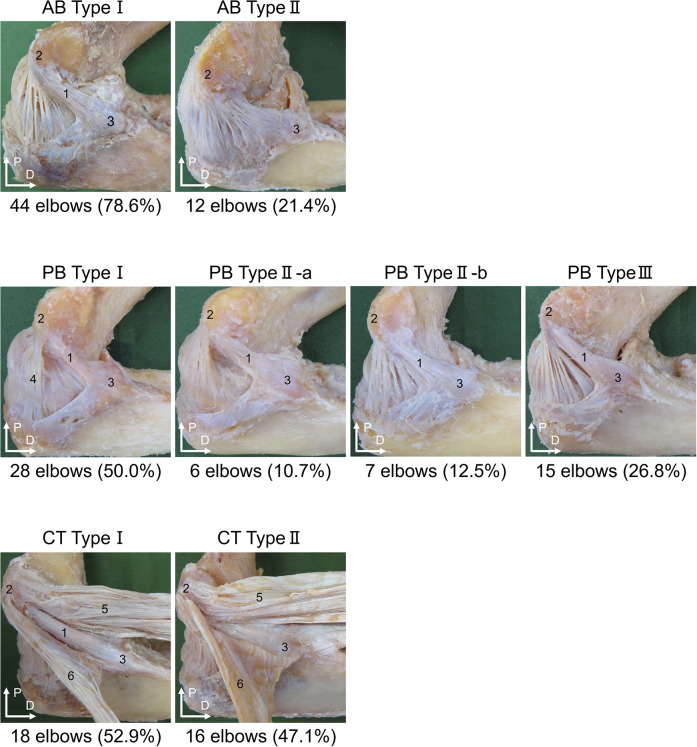
Results: The AB was classified as type I (44 elbows; 78.6%), can be separated as a single bundle, or type II (12 elbows; 21.4%), cannot be separated from the PB and joint capsule. The PB was classified as type I (28 elbows; 50.0%), can be separated as a single bundle; type IIa (6 elbows; 10.7%), posterior edge cannot be separated; type IIb (7 elbows; 12.5%), anterior edge cannot be separated; or type III (15 elbows; 26.8%), cannot be separated from the joint capsule. The CT was classified as type I (18 elbows; 52.9%), can be separated from the AB, or type II (16 elbows; 47.1%), cannot be separated from the AB. Significant differences in frequencies of AB, PB, and CT types were identified between men and women. Morphological features were measured only for type I of each structure, and reliability was almost perfect.
Conclusion: These results suggest that the AB, PB, and CT each can be classified into an independent form and an unclear form. Presence of the unclear form was suggested as one factor contributing to morphological variation.
Clinical relevance: This study may provide basic information for clarifying functional roles of the AB, PB, and CT.
Keywords: anatomy; baseball; elbow; ulnar collateral ligament injury.
© The Author(s) 2020.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI grant No. JP19K11358 and a grant-in-aid program from Niigata University of Health and Welfare. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Cage DJ, Abrams RA, Callahan JJ, Botte MJ. Soft tissue attachments of the ulnar coronoid process: an anatomic study with radiographic correlation. Clin Orthop Relat Res. 1995;320:154–158. - PubMed
-
- Ciccotti MG, Pollack KM, Ciccotti MC, et al. Elbow injuries in professional baseball: epidemiological findings from the Major League Baseball Injury Surveillance System. Am J Sports Med. 2017;45(10):2319–2328. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
