

Expanding Access to Perinatal Depression Treatment in Kenya Through Automated Psychological Support: Development and Usability Study
- PMID: 33016883
- PMCID: PMC7573703
- DOI: 10.2196/17895
Expanding Access to Perinatal Depression Treatment in Kenya Through Automated Psychological Support: Development and Usability Study
Abstract
Background: Depression during pregnancy and in the postpartum period is associated with poor outcomes for women and their children. Although effective interventions exist for common mental disorders that occur during pregnancy and the postpartum period, most cases in low- and middle-income countries go untreated because of a lack of trained professionals. Task-sharing models such as the Thinking Healthy Program have shown potential in feasibility and efficacy trials as a strategy for expanding access to treatment in low-resource settings; however, there are significant barriers to scale-up. We address this gap by adapting Thinking Healthy for automated delivery via a mobile phone. This new intervention, Healthy Moms, uses an existing artificial intelligence system called Tess (Zuri in Kenya) to drive conversations with users.
Objective: This prepilot study aims to gather preliminary data on the Healthy Moms perinatal depression intervention to learn how to build and test a more robust service.
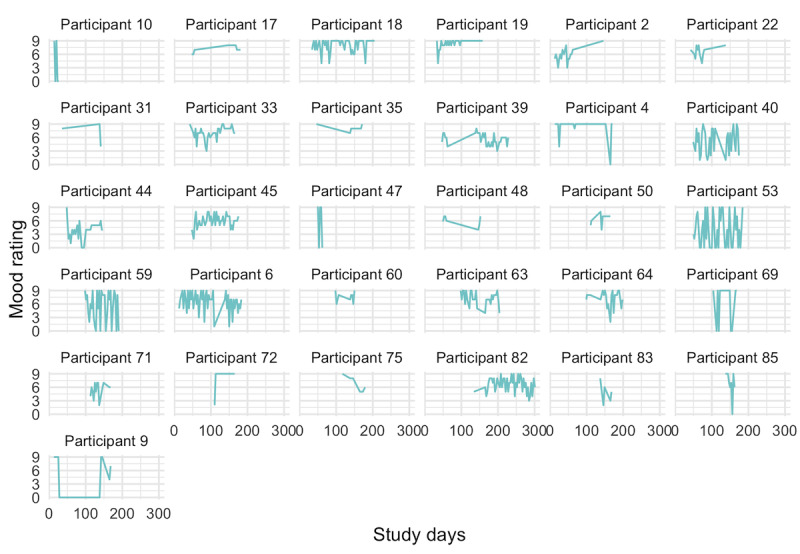
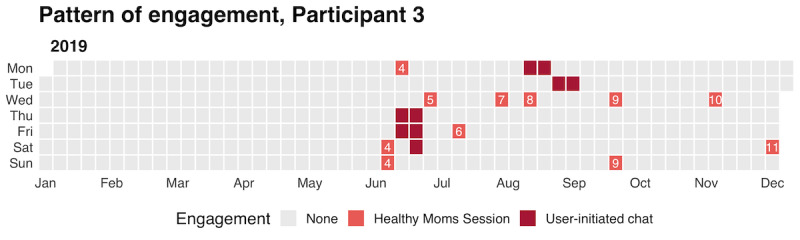
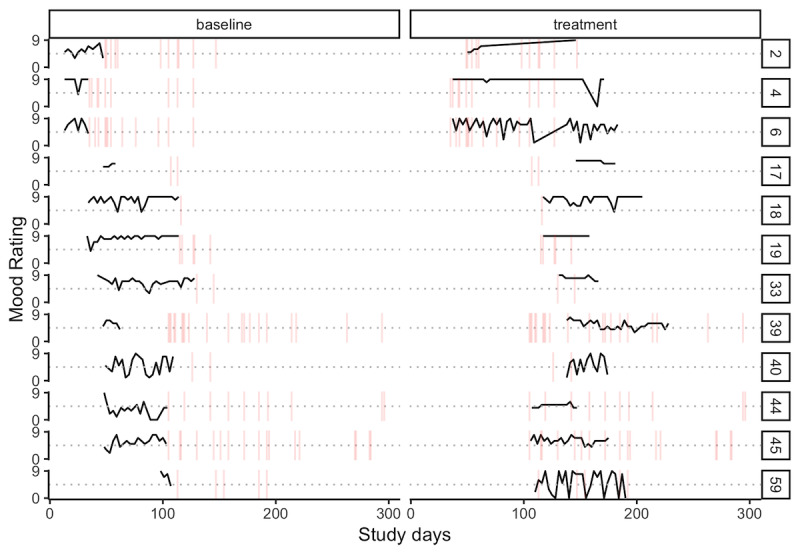
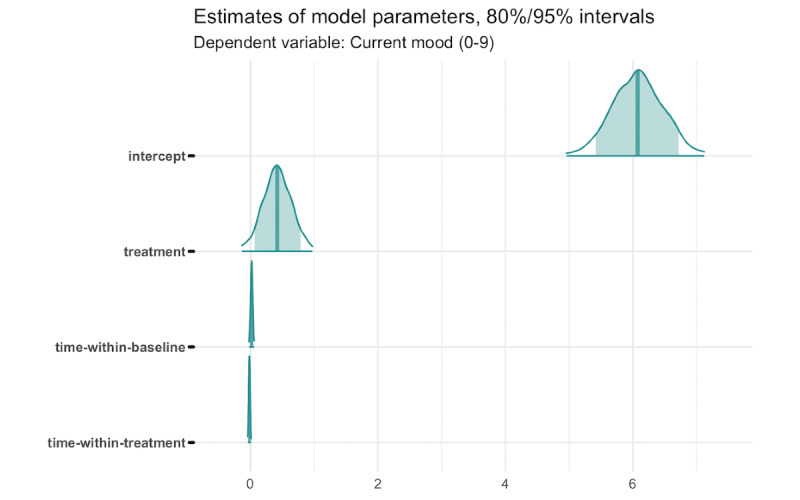
Methods: We conducted a single-case experimental design with pregnant women and new mothers recruited from public hospitals outside of Nairobi, Kenya. We invited these women to complete a brief, automated screening delivered via text messages to determine their eligibility. Enrolled participants were randomized to a 1- or 2-week baseline period and then invited to begin using Zuri. We prompted participants to rate their mood via SMS text messaging every 3 days during the baseline and intervention periods, and we used these preliminary repeated measures data to fit a linear mixed-effects model of response to treatment. We also reviewed system logs and conducted in-depth interviews with participants to study engagement with the intervention, feasibility, and acceptability.
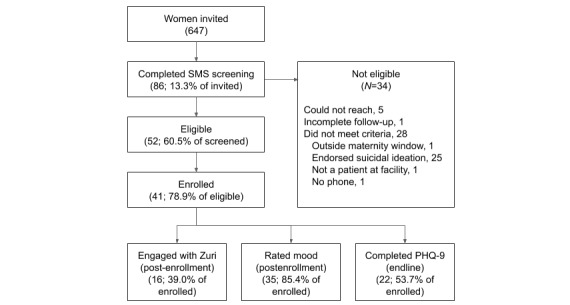
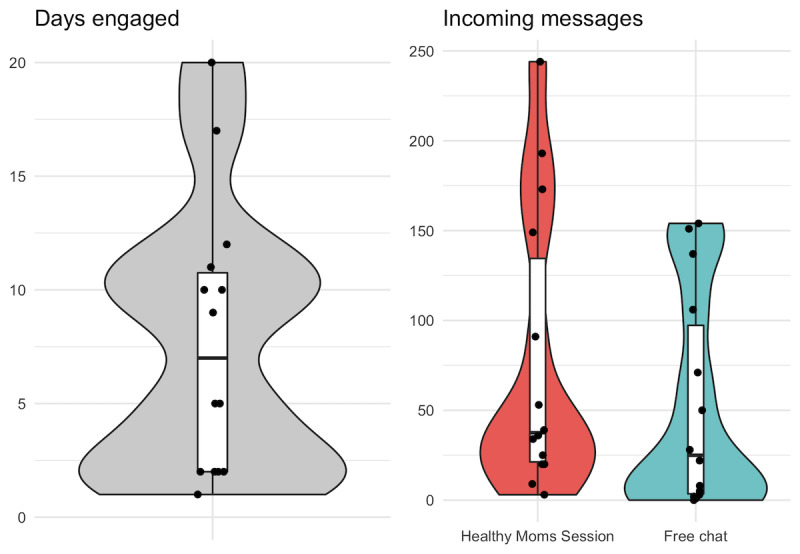
Results: We invited 647 women to learn more about Zuri: 86 completed our automated SMS screening and 41 enrolled in the study. Most of the enrolled women submitted at least 3 mood ratings (31/41, 76%) and sent at least 1 message to Zuri (27/41, 66%). A third of the sample engaged beyond registration (14/41, 34%). On average, women who engaged post registration started 3.4 (SD 3.2) Healthy Moms sessions and completed 3.1 (SD 2.9) of the sessions they started. Most interviewees who tried Zuri reported having a positive attitude toward the service and expressed trust in Zuri. They also attributed positive life changes to the intervention. We estimated that using this alpha version of Zuri may have led to a 7% improvement in mood.
Conclusions: Zuri is feasible to deliver via SMS and was acceptable to this sample of pregnant women and new mothers. The results of this prepilot study will serve as a baseline for future studies in terms of recruitment, data collection, and outcomes.
International registered report identifier (irrid): RR2-10.2196/11800.
Keywords: Kenya; artificial intelligence; depression; mental health; mobile phone; telemedicine; text messaging.
©Eric P Green, Yihuan Lai, Nicholas Pearson, Sathyanath Rajasekharan, Michiel Rauws, Angela Joerin, Edith Kwobah, Christine Musyimi, Rachel M Jones, Chaya Bhat, Antonia Mulinge, Eve S Puffer. Originally published in JMIR Formative Research (http://formative.jmir.org), 05.10.2020.
Conflict of interest statement
Conflicts of Interest: MR is the CEO and Founder of X2AI and created Tess. AJ is an employee of X2AI. EG is an unpaid advisor to the X2AI Ethical Advisory Board and has no financial stake in the company.
Figures
Similar articles
-
Expanding Access to Depression Treatment in Kenya Through Automated Psychological Support: Protocol for a Single-Case Experimental Design Pilot Study.JMIR Res Protoc. 2019 Apr 29;8(4):e11800. doi: 10.2196/11800. JMIR Res Protoc. 2019. PMID: 31033448 Free PMC article.
-
The Development and Evaluation of a Text Message Program to Prevent Perceived Insufficient Milk Among First-Time Mothers: Retrospective Analysis of a Randomized Controlled Trial.JMIR Mhealth Uhealth. 2020 Apr 29;8(4):e17328. doi: 10.2196/17328. JMIR Mhealth Uhealth. 2020. PMID: 32347815 Free PMC article. Clinical Trial.
-
Personalized Text Messages and Automated Calls for Improving Vaccine Coverage Among Children in Pakistan: Protocol for a Community-Based Cluster Randomized Clinical Trial.JMIR Res Protoc. 2019 May 30;8(5):e12851. doi: 10.2196/12851. JMIR Res Protoc. 2019. PMID: 31148544 Free PMC article.
-
Feasibility and impact of a mental health chatbot on postpartum mental health: a randomized controlled trial.AJOG Glob Rep. 2023 Mar 29;3(3):100165. doi: 10.1016/j.xagr.2023.100165. eCollection 2023 Aug. AJOG Glob Rep. 2023. PMID: 37560011 Free PMC article.
-
Assessing Mobile Phone Access and Perceptions for Texting-Based mHealth Interventions Among Expectant Mothers and Child Caregivers in Remote Regions of Northern Kenya: A Survey-Based Descriptive Study.JMIR Public Health Surveill. 2017 Jan 30;3(1):e5. doi: 10.2196/publichealth.5386. JMIR Public Health Surveill. 2017. PMID: 28137702 Free PMC article.
Cited by
-
Health-focused conversational agents in person-centered care: a review of apps.NPJ Digit Med. 2022 Feb 17;5(1):21. doi: 10.1038/s41746-022-00560-6. NPJ Digit Med. 2022. PMID: 35177772 Free PMC article. Review.
-
Interventions to increase help-seeking for mental health care in low- and middle-income countries: A systematic review.PLOS Glob Public Health. 2023 Sep 13;3(9):e0002302. doi: 10.1371/journal.pgph.0002302. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37703225 Free PMC article.
-
Digital health for all: How digital health could reduce inequality and increase universal health coverage.Digit Health. 2023 Jul 7;9:20552076231185434. doi: 10.1177/20552076231185434. eCollection 2023 Jan-Dec. Digit Health. 2023. PMID: 37434727 Free PMC article.
-
Debate and Dilemmas Regarding Generative AI in Mental Health Care: Scoping Review.Interact J Med Res. 2024 Aug 12;13:e53672. doi: 10.2196/53672. Interact J Med Res. 2024. PMID: 39133916 Free PMC article.
-
Scaling up community-delivered mental health support and care: A landscape analysis.Front Public Health. 2022 Dec 8;10:992222. doi: 10.3389/fpubh.2022.992222. eCollection 2022. Front Public Health. 2022. PMID: 36568763 Free PMC article. Review.
References
-
- Field T. Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behav Dev. 2010 Feb;33(1):1–6. doi: 10.1016/j.infbeh.2009.10.005. http://europepmc.org/abstract/MED/19962196 S0163-6383(09)00097-6 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
