

Global, regional, and national burden of ischaemic heart disease and its attributable risk factors, 1990-2017: results from the Global Burden of Disease Study 2017
- PMID: 33017008
- PMCID: PMC8728029
- DOI: 10.1093/ehjqcco/qcaa076
Global, regional, and national burden of ischaemic heart disease and its attributable risk factors, 1990-2017: results from the Global Burden of Disease Study 2017
Abstract
Aims: The aim of this study was to estimate the burden and risk factors for ischaemic heart disease (IHD) in 195 countries and territories from 1990 to 2017.
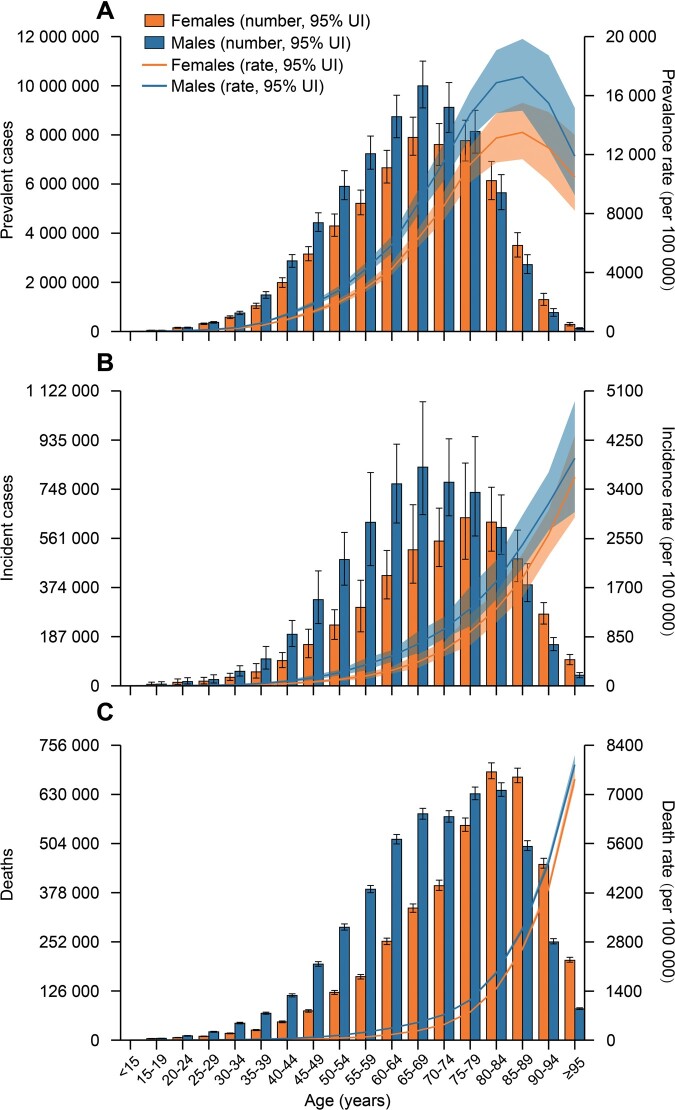
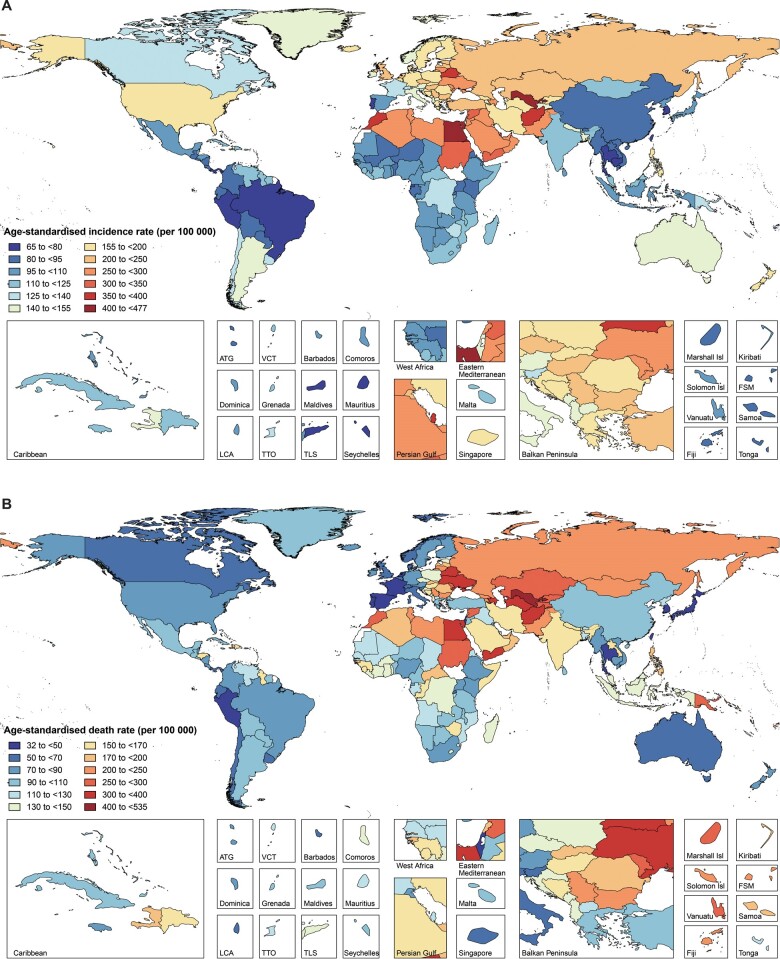
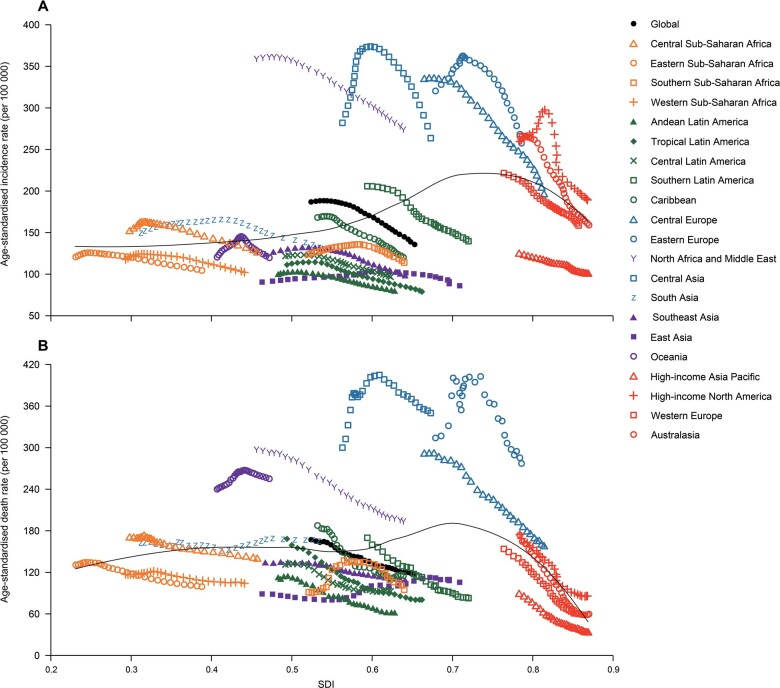
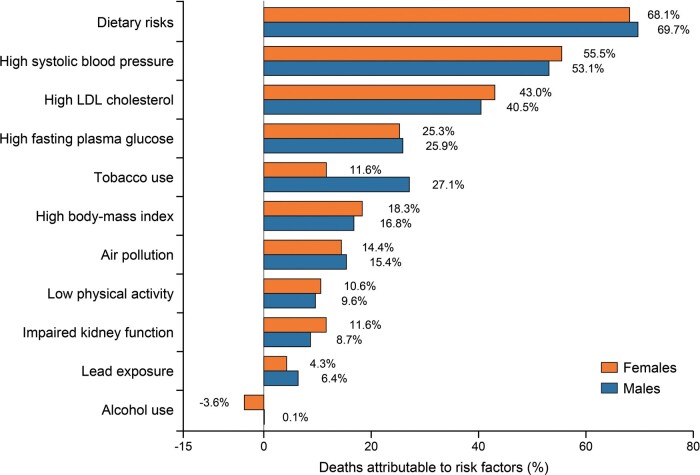
Methods and results: Data from the Global Burden of Disease Study 2017 were used. Prevalence, incidence, deaths, years lived with disability (YLDs), and years of life lost (YLLs) were metrics used to measure IHD burden. Population attributable fraction was used to estimate the proportion of IHD deaths attributable to potentially modifiable risk factors. Globally, in 2017, 126.5 million [95% uncertainty interval (UI) 118.6 to 134.7] people lived with IHD and 10.6 million (95% UI 9.6 to 11.8) new IHD cases occurred, resulting in 8.9 million (95% UI 8.8 to 9.1) deaths, 5.3 million (95% UI 3.7 to 7.2) YLDs, and 165.0 million (95% UI 162.2 to 168.6) YLLs. Between 1990 and 2017, despite the decrease in age-standardized rates, the global numbers of these burden metrics of IHD have significantly increased. The burden of IHD in 2017 and its temporal trends from 1990 to 2017 varied widely by geographic location. Among all potentially modifiable risk factors, age-standardized IHD deaths worldwide were primarily attributable to dietary risks, high systolic blood pressure, high LDL cholesterol, high fasting plasma glucose, tobacco use, and high body mass index in 2017.
Conclusion: Our results suggested that IHD remains a major public health challenge worldwide. More effective and targeted strategies aimed at implementing cost-effective interventions and addressing modifiable risk factors are urgently needed, particularly in geographies with high or increasing burden.
Keywords: Epidemiology; Global heath; Ischaemic heart disease; Risk factor.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP et al. ; On behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2020 update: a report from the American Heart Association. Circulation 2020;141:e139–e596. - PubMed
-
- Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart failure. Int J Cardiol 2014;171:368–376. - PubMed
