

Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19
- PMID: 33017083
- PMCID: PMC7675597
- DOI: 10.1111/jce.14770
Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19
Abstract
Introduction: The impact of atrial arrhythmias on coronavirus disease 2019 (COVID-19)-associated outcomes are unclear. We sought to identify prevalence, risk factors and outcomes associated with atrial arrhythmias among patients hospitalized with COVID-19.
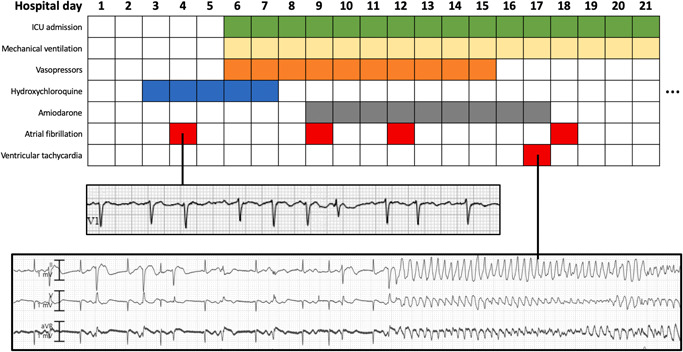
Methods: An observational cohort study of 1053 patients with severe acute respiratory syndrome coronavirus 2 infection admitted to a quaternary care hospital and a community hospital was conducted. Data from electrocardiographic and telemetry were collected to identify atrial fibrillation (AF) or atrial flutter/tachycardia (AFL). The association between atrial arrhythmias and 30-day mortality was assessed with multivariable analysis.
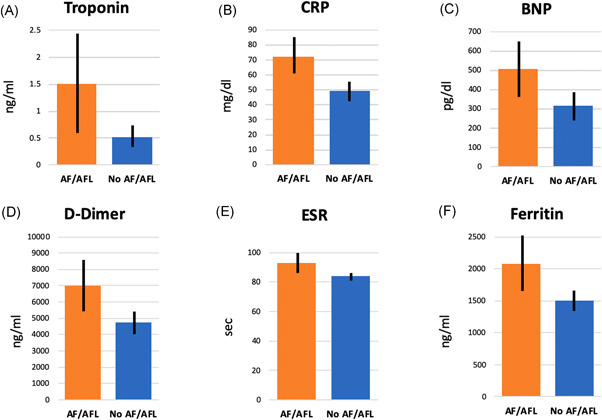
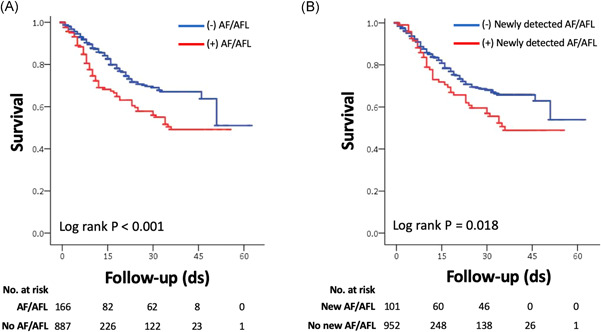
Results: Mean age of patients was 62 ± 17 years and 62% were men. Atrial arrhythmias were identified in 166 (15.8%) patients, with AF in 154 (14.6%) patients and AFL in 40 (3.8%) patients. Newly detected atrial arrhythmias occurred in 101 (9.6%) patients. Age, male sex, prior AF, renal disease, and hypoxia on presentation were independently associated with AF/AFL occurrence. Compared with patients without AF/AFL, patients with AF/AFL had significantly higher levels of troponin, B-type natriuretic peptide, C-reactive protein, ferritin and d-dimer. Mortality was significantly higher among patients with AF/AFL (39.2%) compared to patients without (13.4%; p < .001). After adjustment for age and co-morbidities, AF/AFL (adjusted odds ratio [OR]: 1.93; p = .007) and newly detected AF/AFL (adjusted OR: 2.87; p < .001) were independently associated with 30-day mortality.
Conclusion: Atrial arrhythmias are common among patients hospitalized with COVID-19. The presence of AF/AFL tracked with markers of inflammation and cardiac injury. Atrial arrhythmias were independently associated with increased mortality.
Keywords: COVID-19; atrial fibrillation; atrial flutter; mortality; outcomes.
© 2020 Wiley Periodicals LLC.
Figures
Comment in
-
Atrial fibrillation and flutter in patients hospitalized for COVID-19: The challenging role of digoxin.J Cardiovasc Electrophysiol. 2021 Mar;32(3):878-879. doi: 10.1111/jce.14894. Epub 2021 Feb 1. J Cardiovasc Electrophysiol. 2021. PMID: 33522637 Free PMC article. No abstract available.
References
-
- Center for Systems Science and Engineering, Johns Hopkins University . COVID dashboard. 2020. https://coronavirus.jhu.edu/map.html. Accessed August 25, 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
