

Persistent metabolomic alterations characterize chronic critical illness after severe trauma
- PMID: 33017357
- PMCID: PMC8011937
- DOI: 10.1097/TA.0000000000002952
Persistent metabolomic alterations characterize chronic critical illness after severe trauma
Abstract
Background: Following trauma, persistent inflammation, immunosuppression, and catabolism may characterize delayed recovery or failure to recover. Understanding the metabolic response associated with these adverse outcomes may facilitate earlier identification and intervention. We characterized the metabolic profiles of trauma victims who died or developed chronic critical illness (CCI) and hypothesized that differences would be evident within 1-week postinjury.
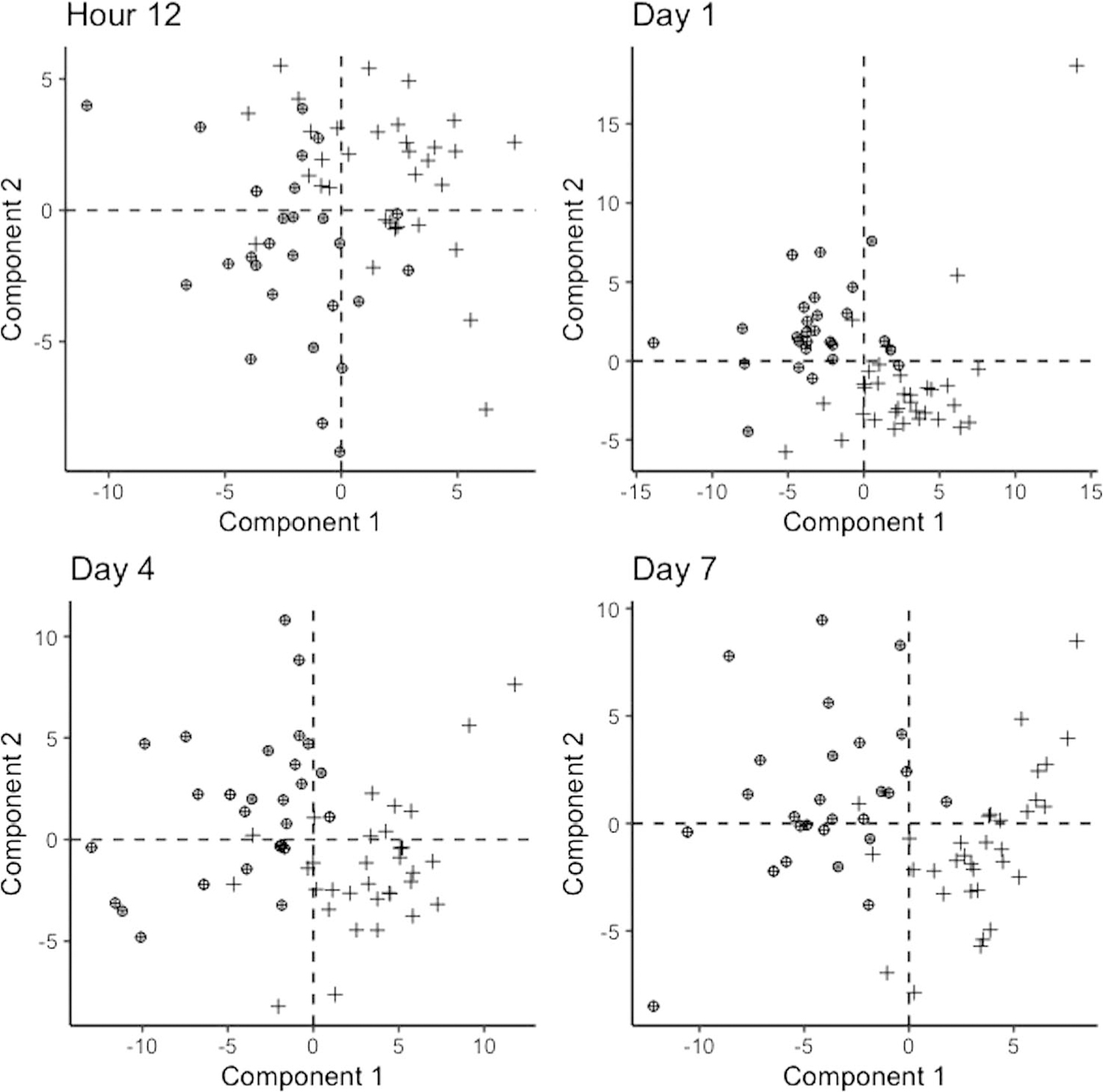
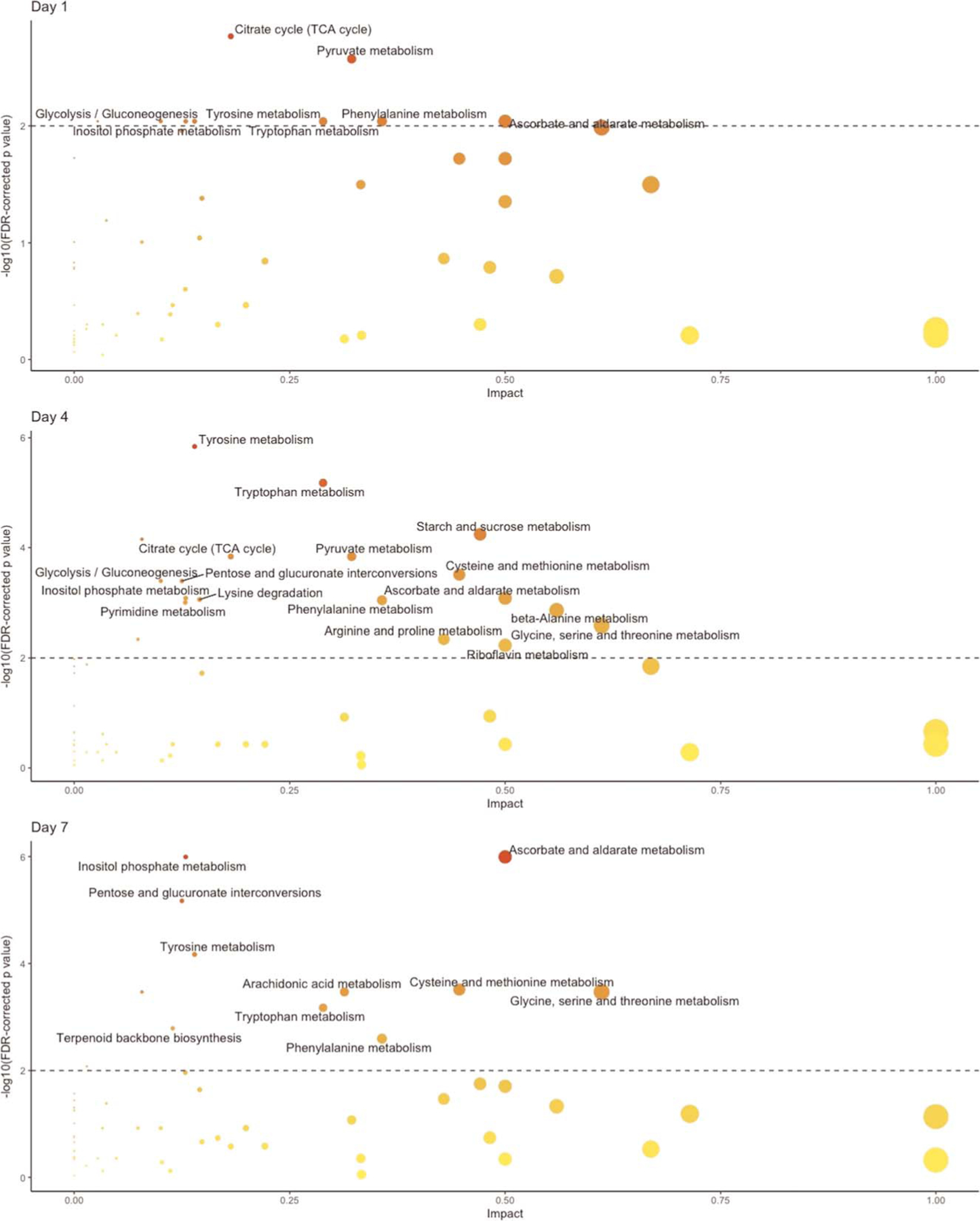
Methods: Venous blood samples from trauma victims with shock who survived at least 7 days were analyzed using mass spectrometry. Subjects who died or developed CCI (intensive care unit length of stay of ≥14 days with persistent organ dysfunction) were compared with subjects who recovered rapidly (intensive care unit length of stay, ≤7 days) and uninjured controls. We used partial least squares discriminant analysis, t tests, linear mixed effects regression, and pathway enrichment analyses to make broad comparisons and identify differences in metabolite concentrations and pathways.
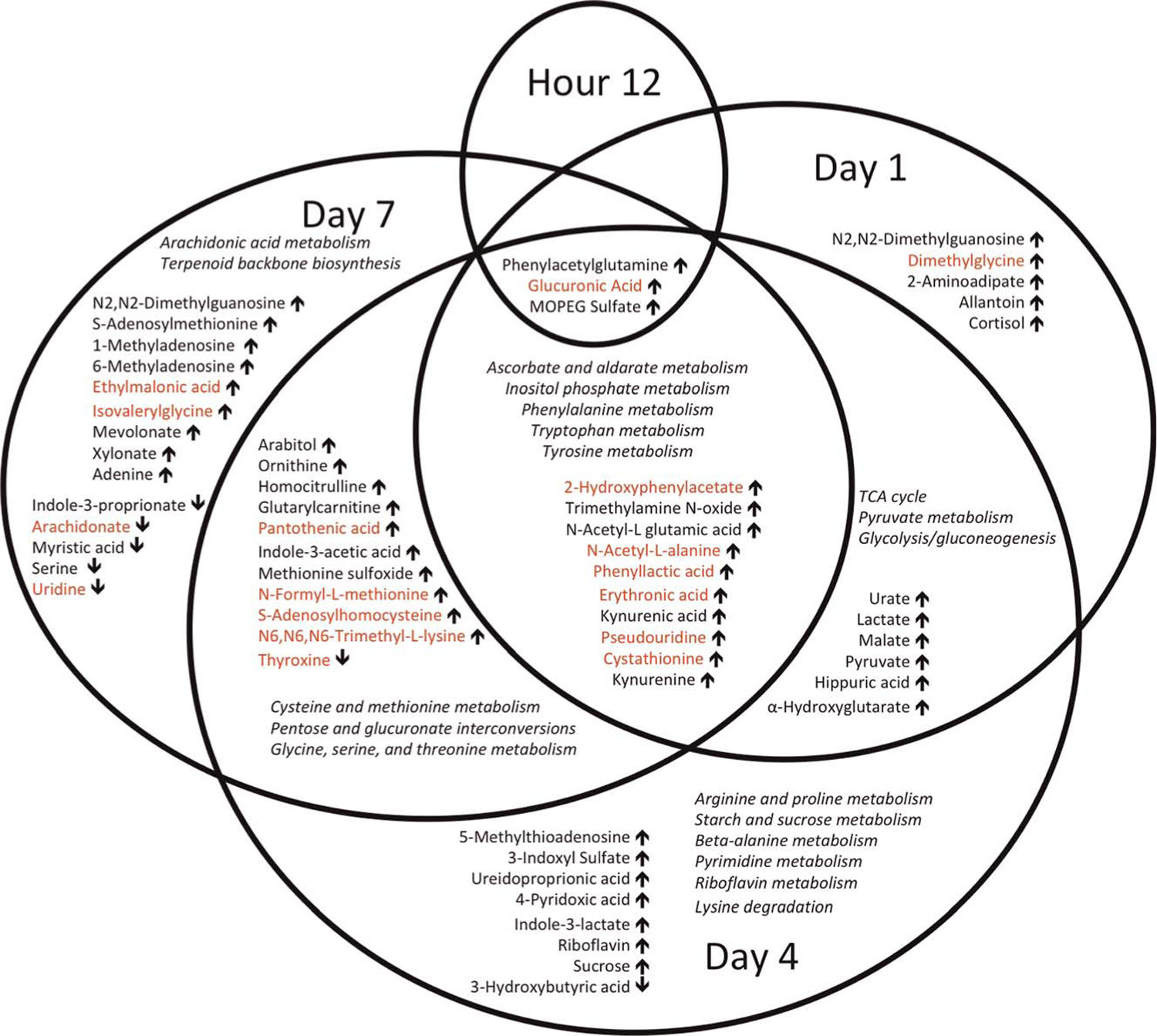
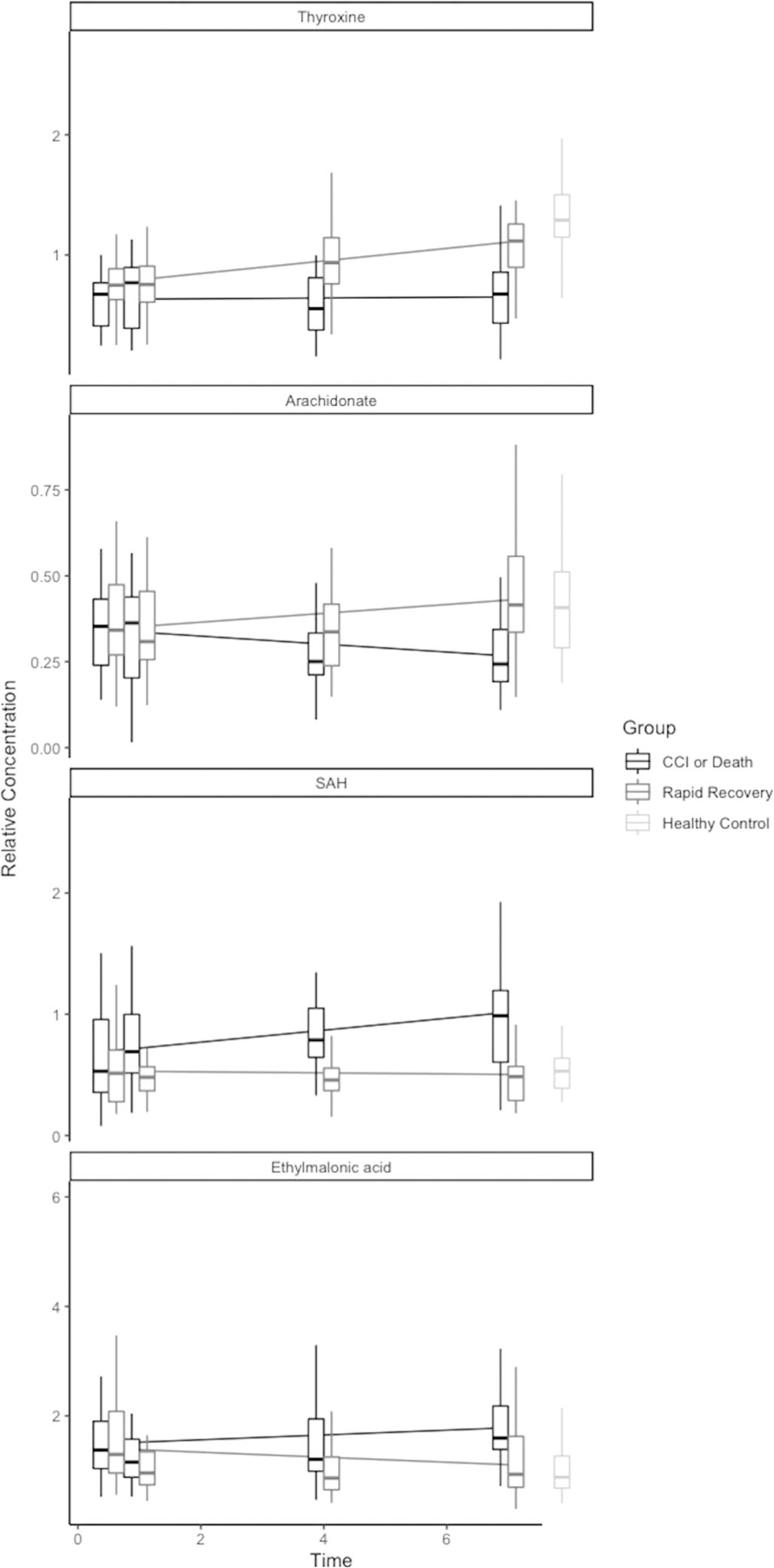
Results: We identified 27 patients who died or developed CCI and 33 who recovered rapidly. Subjects were predominantly male (65%) with a median age of 53 years and Injury Severity Score of 36. Healthy controls (n = 48) had similar age and sex distributions. Overall, from the 163 metabolites detected in the samples, 56 metabolites and 21 pathways differed between injury outcome groups, and partial least squares discriminant analysis models distinguished injury outcome groups as early as 1-day postinjury. Differences were observed in tryptophan, phenylalanine, and tyrosine metabolism; metabolites associated with oxidative stress via methionine metabolism; inflammatory mediators including kynurenine, arachidonate, and glucuronic acid; and products of the gut microbiome including indole-3-propionate.
Conclusions: The metabolic profiles in subjects who ultimately die or develop CCI differ from those who have recovered. In particular, we have identified differences in markers of inflammation, oxidative stress, amino acid metabolism, and alterations in the gut microbiome. Targeted metabolomics has the potential to identify important metabolic changes postinjury to improve early diagnosis and targeted intervention.
Level of evidence: Prognostic/epidemiologic, level III.
Copyright © 2020 American Association for the Surgery of Trauma.
Conflict of interest statement
DISCLOSURE
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
