

Filling the gaps on stroke research: Focus on inflammation and immunity
- PMID: 33017613
- PMCID: PMC7531595
- DOI: 10.1016/j.bbi.2020.09.025
Filling the gaps on stroke research: Focus on inflammation and immunity
Abstract
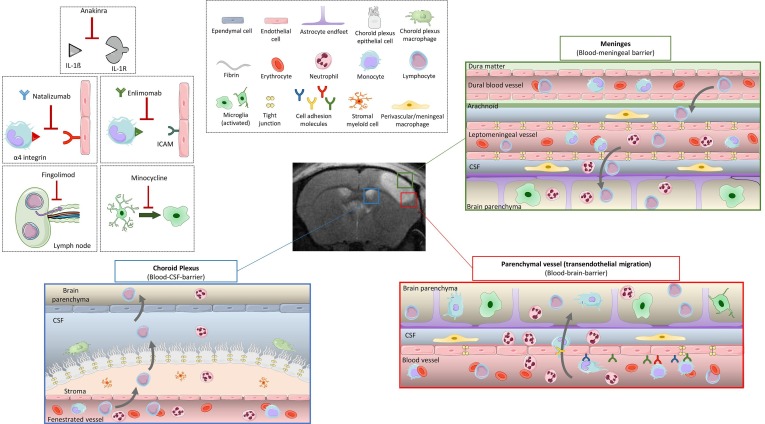
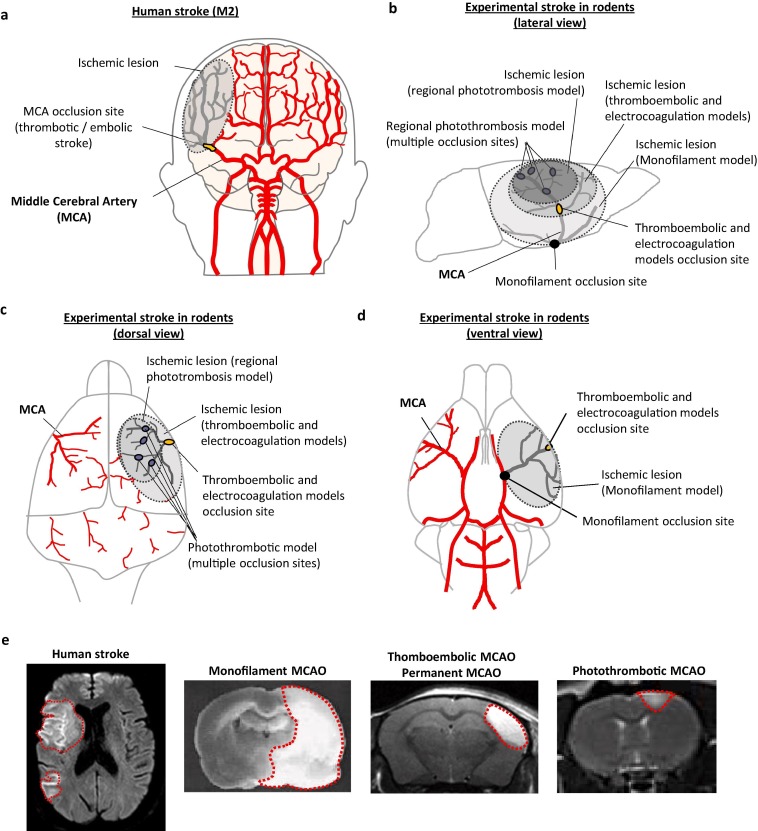
For the last two decades, researchers have placed hopes in a new era in which a combination of reperfusion and neuroprotection would revolutionize the treatment of stroke. Nevertheless, despite the thousands of papers available in the literature showing positive results in preclinical stroke models, randomized clinical trials have failed to show efficacy. It seems clear now that the existing data obtained in preclinical research have depicted an incomplete picture of stroke pathophysiology. In order to ameliorate bench-to-bed translation, in this review we first describe the main actors on stroke inflammatory and immune responses based on the available preclinical data, highlighting the fact that the link between leukocyte infiltration, lesion volume and neurological outcome remains unclear. We then describe what is known on neuroinflammation and immune responses in stroke patients, and summarize the results of the clinical trials on immunomodulatory drugs. In order to understand the gap between clinical trials and preclinical results on stroke, we discuss in detail the experimental results that served as the basis for the summarized clinical trials on immunomodulatory drugs, focusing on (i) experimental stroke models, (ii) the timing and selection of outcome measuring, (iii) alternative entry routes for leukocytes into the ischemic region, and (iv) factors affecting stroke outcome such as gender differences, ageing, comorbidities like hypertension and diabetes, obesity, tobacco, alcohol consumption and previous infections like Covid-19. We can do better for stroke treatment, especially when targeting inflammation following stroke. We need to re-think the design of stroke experimental setups, notably by (i) using clinically relevant models of stroke, (ii) including both radiological and neurological outcomes, (iii) performing long-term follow-up studies, (iv) conducting large-scale preclinical stroke trials, and (v) including stroke comorbidities in preclinical research.
Keywords: Clinical trials; Experimental models; Immune response; Inflammation; Ischemic stroke; Translational research.
Copyright © 2020. Published by Elsevier Inc.
Figures
Similar articles
-
Immune Responses and Anti-inflammatory Strategies in a Clinically Relevant Model of Thromboembolic Ischemic Stroke with Reperfusion.Transl Stroke Res. 2020 Jun;11(3):481-495. doi: 10.1007/s12975-019-00733-8. Epub 2019 Sep 14. Transl Stroke Res. 2020. PMID: 31522409
-
Impact of aging and comorbidities on ischemic stroke outcomes in preclinical animal models: A translational perspective.Exp Neurol. 2021 Jan;335:113494. doi: 10.1016/j.expneurol.2020.113494. Epub 2020 Oct 7. Exp Neurol. 2021. PMID: 33035516 Free PMC article. Review.
-
Preclinical stroke research--advantages and disadvantages of the most common rodent models of focal ischaemia.Br J Pharmacol. 2011 Oct;164(4):1062-78. doi: 10.1111/j.1476-5381.2011.01398.x. Br J Pharmacol. 2011. PMID: 21457227 Free PMC article. Review.
-
A new era for stroke therapy: Integrating neurovascular protection with optimal reperfusion.J Cereb Blood Flow Metab. 2018 Dec;38(12):2073-2091. doi: 10.1177/0271678X18798162. Epub 2018 Sep 7. J Cereb Blood Flow Metab. 2018. PMID: 30191760 Free PMC article. Review.
-
Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke.Stroke. 2003 Aug;34(8):e109-37. doi: 10.1161/01.STR.0000082721.62796.09. Epub 2003 Jul 17. Stroke. 2003. PMID: 12869717
Cited by
-
Network pharmacology and molecular docking-based analysis of protective mechanism of MLIF in ischemic stroke.Front Cardiovasc Med. 2022 Nov 18;9:1071533. doi: 10.3389/fcvm.2022.1071533. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36465453 Free PMC article.
-
Elucidating the Synergistic Effect of Multiple Chinese Herbal Prescriptions in the Treatment of Post-stroke Neurological Damage.Front Pharmacol. 2022 Mar 9;13:784242. doi: 10.3389/fphar.2022.784242. eCollection 2022. Front Pharmacol. 2022. PMID: 35355727 Free PMC article.
-
Exacerbated VEGF up-regulation accompanies diabetes-aggravated hemorrhage in mice after experimental cerebral ischemia and delayed reperfusion.Neural Regen Res. 2022 Jul;17(7):1566-1575. doi: 10.4103/1673-5374.330612. Neural Regen Res. 2022. PMID: 34916442 Free PMC article.
-
Humanized mouse model reveals T cell ANXA2 as a potential therapeutic target in ischemic stroke.iScience. 2025 Apr 2;28(5):112302. doi: 10.1016/j.isci.2025.112302. eCollection 2025 May 16. iScience. 2025. PMID: 40641552 Free PMC article.
-
Neuroprotective Effects of Tryptanthrin-6-Oxime in a Rat Model of Transient Focal Cerebral Ischemia.Pharmaceuticals (Basel). 2023 Jul 25;16(8):1057. doi: 10.3390/ph16081057. Pharmaceuticals (Basel). 2023. PMID: 37630972 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
