

Confirmed cases of Neuroborreliosis with involvement of peripheral nervous system: Description of a cohort
- PMID: 33019390
- PMCID: PMC7535703
- DOI: 10.1097/MD.0000000000021986
Confirmed cases of Neuroborreliosis with involvement of peripheral nervous system: Description of a cohort
Abstract
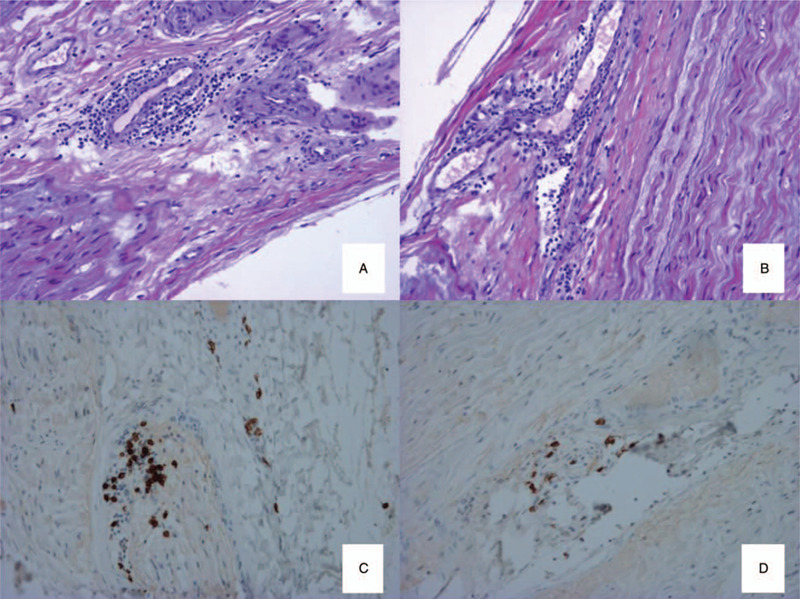
The manifestations of borreliosis in the peripheral nervous system (PNS) remain poorly described. As the symptoms of neuroborreliosis can be reversed with timely introduction of antibiotics, early identification could avoid unnecessary axonal loss. Our aim was to describe the characteristics of confirmed neuroborreliosis cases involving the PNS diagnosed between 2007 and 2017 in our neuromuscular disease center in a nonendemic area (La Pitié-Salpêtrière Hospital, Paris, France).Neuroborreliosis was defined as follows: compatible neurological symptoms without other cause of neuropathy; cerebrospinal fluid and serum analysis (positive serological tests with ELISA, confirmed by Western Blot); and improvement of symptoms with adapted antibiotherapy. All the patients consulting in our center between 2007 and 2017 underwent electrophysiological study.Sixteen confirmed cases of neuroborreliosis involving the PNS were included: 10 cases of meningoradiculoneuritis, 4 of axonal neuropathy, and 2 of demyelinating neuropathy (one acute and one chronic). Only 4 (25%) patients reported tick bites. Meningoradiculoneuritis was characterized by lymphocytic meningitis, intense pain, cranial nerve palsy, and contrast enhancement of nerve roots on imagery. The patients with axonal neuropathy presented sensory symptoms with intense pain but no motor deficit and meningitis was rare. Nerve biopsy of 1 patient revealed lymphocytic vasculitis. Electrophysiological testing showed sensory or sensorimotor axonal neuropathy (3 subacute and 1 chronic) of the lower limbs, with asymmetrical neuropathy in 1 patients, symmetrical neuropathy in one and monomelic sensory mononeuritis multiplex in another. We also found 1 case of acute demyelinating neuropathy, treated with antibiotherapy and immunoglobulins, and 1 chronic demyelinating neuropathy. Overall, diaphragmatic paralysis was frequent (18.6%). Antibiotherapy (mostly ceftriaxone 3-4 weeks) resulted in symptom resolution.This series gives an updated overview of the peripheral complications of neuroborreliosis to help identify this disease so that timely treatment could avoid axonal loss.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Mygland A, Skarpaas T, Ljøstad U. Chronic polyneuropathy and Lyme disease. Eur J Neurol 2006;13:1213–5. - PubMed
-
- Akbik F, Matiello M, Piquet A, et al. Bibrachial plegia due to Lyme radiculopoliomyelitis-myelitis. J Neurol Sci 2017;378:1–2. - PubMed
-
- Halperin JJ. Neuroborreliosis. J Neurol 2017;264:1292–7. - PubMed
-
- Cuvelier ML, Léonard P, Rikir E, et al. Neuroborreliosis [Article in French]. Rev Med Liege 2008;63:349–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
