

Targeted Molecular Therapeutics for Bladder Cancer-A New Option beyond the Mixed Fortunes of Immune Checkpoint Inhibitors?
- PMID: 33019653
- PMCID: PMC7582582
- DOI: 10.3390/ijms21197268
Targeted Molecular Therapeutics for Bladder Cancer-A New Option beyond the Mixed Fortunes of Immune Checkpoint Inhibitors?
Abstract
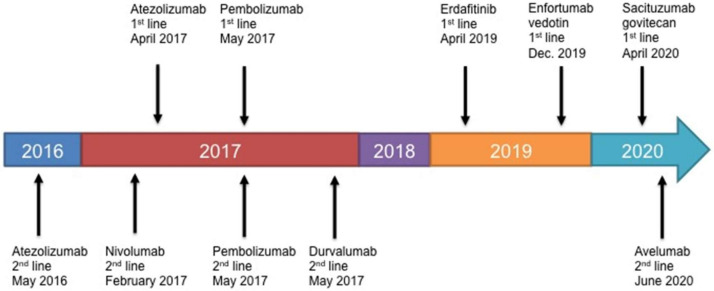
The fact that there are now five immune checkpoint inhibitor (ICI) monoclonal antibodies approved since 2016 that target programmed cell death protein 1 or programmed death ligand-1 for the treatment of metastatic and refractory bladder cancer is an outstanding achievement. Although patients can display pronounced responses that extend survival when treated with ICIs, the main benefit of these drugs compared to traditional chemotherapy is that they are better tolerated and result in reduced adverse events (AEs). Unfortunately, response rates to ICI treatment are relatively low and, these drugs are expensive and have a high economic burden. As a result, their clinical efficacy/cost-value relationship is debated. Long sought after targeted molecular therapeutics have now emerged and are boasting impressive response rates in heavily pre-treated, including ICI treated, patients with metastatic bladder cancer. The antibody-drug conjugates (ADCs) enfortumab vedotin (EV) and sacituzumab govitecan (SG) have demonstrated the ability to provide objective response rates (ORRs) of 44% and 31% in patients with bladder tumor cells that express Nectin-4 and Trop-2, respectively. As a result, EV was approved by the U.S. Food and Drug Administration for the treatment of patients with advanced or metastatic bladder cancer who have previously received ICI and platinum-containing chemotherapy. SG has been granted fast track designation. The small molecule Erdafitinib was recently approved for the treatment of patients with advanced or metastatic bladder cancer with genetic alterations in fibroblast growth factor receptors that have previously been treated with a platinum-containing chemotherapy. Erdafitinib achieved an ORR of 40% in patients including a proportion who had previously received ICI therapy. In addition, these targeted drugs are sufficiently tolerated or AEs can be appropriately managed. Hence, the early performance in clinical effectiveness of these targeted drugs are substantially increased relative to ICIs. In this article, the most up to date follow-ups on treatment efficacy and AEs of the ICIs and targeted therapeutics are described. In addition, drug price and cost-effectiveness are described. For best overall value taking into account clinical effectiveness, price and cost-effectiveness, results favor avelumab and atezolizumab for ICIs. Although therapeutically promising, it is too early to determine if the described targeted therapeutics provide the best overall value as cost-effectiveness analyses have yet to be performed and long-term follow-ups are needed. Nonetheless, with the arrival of targeted molecular therapeutics and their increased effectiveness relative to ICIs, creates a potential novel paradigm based on 'targeting' for affecting clinical practice for metastatic bladder cancer treatment.
Keywords: antibodies; antibody-drug conjugates; bladder cancer; cost-effectiveness; enfortumab vedotin; erdafitinib; immune checkpoint inhibitors; sacituzumab govitecan.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bladder Cancer Fact Sheet. [(accessed on 24 July 2020)]; Available online: https://gco.iarc.fr/today/data/factsheets/cancers/30-Bladder-fact-sheet.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
