

Fatal outcome of anti-MDA5 juvenile dermatomyositis in a paediatric COVID-19 patient: a case report
- PMID: 33019894
- PMCID: PMC8344517
- DOI: 10.1080/24725625.2020.1832755
Fatal outcome of anti-MDA5 juvenile dermatomyositis in a paediatric COVID-19 patient: a case report
Abstract
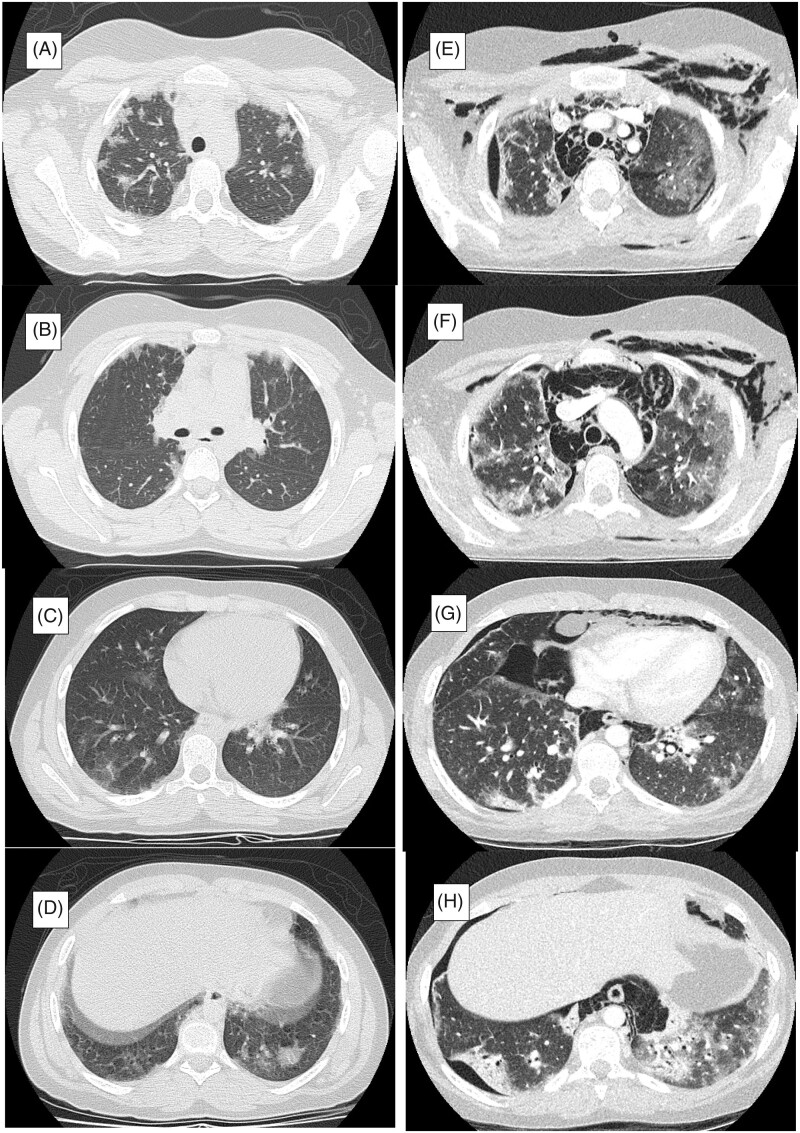
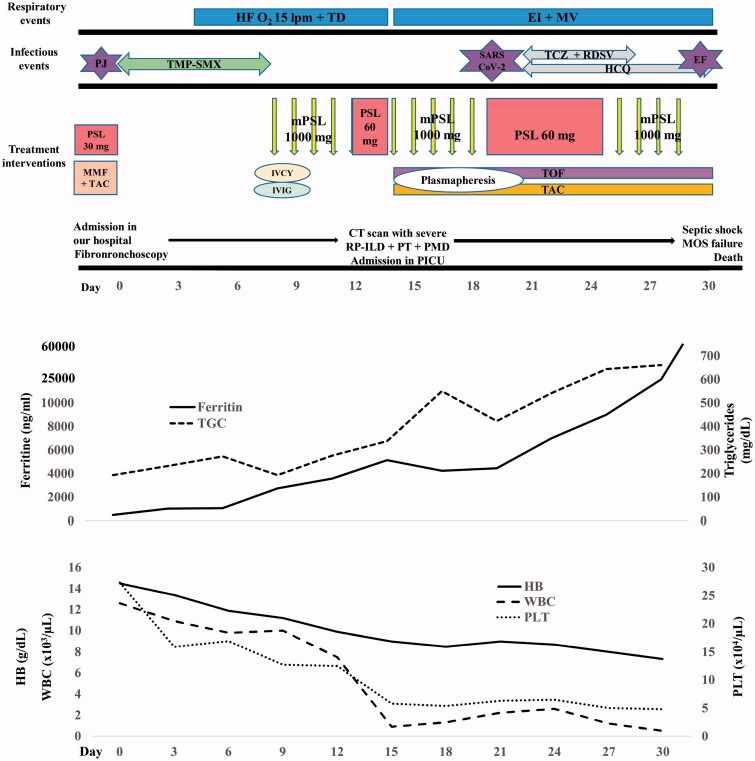
Anti-melanoma differentiation-associated gene 5 juvenile dermatomyositis (anti-MDA5 JDM) is associated with high risk of developing rapidly progressive interstitial lung disease (RP-ILD). Here we report an 11-year-old girl with anti-MDA5 JDM and RP-ILD which led to a fatal outcome, further aggravated by SARS-CoV-2 infection. She was referred to our hospital after being diagnosed with anti-MDA5 JDM and respiratory failure due to RP-ILD. On admission, fibrobronchoscopy with bronchoalveolar lavage (BAL) revealed Pneumocystis jirovecii infection so treatment with intravenous trimethoprim-sulfamethoxazole was initiated. Due to RP-ILD worsening, immunosuppressive therapy was intensified using methylprednisolone pulses, cyclophosphamide, tofacitinib and intravenous immunoglobulin without response. She developed severe hypoxemic respiratory failure, pneumomediastinum and pneumothorax, further complicated with severe RP-ILD and cervical subcutaneous emphysema. Three real-time RT-PCR for SARS-CoV-2 were made with a negative result. In addition, she was complicated with a secondary hemophagocytic lymphohistiocytosis and a fourth real-time PCR for SARS-CoV-2 performed in BAS sample was positive. Despite aggressive treatment of RP-ILD due to anti-MDA5 JDM, there was no improvement of respiratory failure in the following days and patient developed refractory septic shock and died. Anti-MDA5 JDM patients with RP-ILD have a poor prognosis with a high mortality rate. For this reason, intensive immunosuppressive therapy is essential including the use of promising drugs such as tofacitinib. COVID-19 in children with underlying health conditions like anti-MDA5 JDM may still be at risk for disease and severe complications.
Keywords: Anti-MDA5; COVID-19; interstitial lung disease (ILD); juvenile dermatomyositis; tofacitinib.
Figures


Similar articles
-
[Three cases report of juvenile dermatomyositis with positive anti-melanoma differentiation associated gene 5 (MDA5) antibody and severe interstitial lung disease and literature review].Zhonghua Er Ke Za Zhi. 2019 Dec 2;57(12):928-933. doi: 10.3760/cma.j.issn.0578-1310.2019.12.007. Zhonghua Er Ke Za Zhi. 2019. PMID: 31795559 Review. Chinese.
-
Successful rituximab treatment for severe rapidly progressive interstitial lung disease with anti-MDA5 antibody-positive juvenile dermatomyositis: a case report and literature review.Pediatr Rheumatol Online J. 2022 Aug 4;20(1):60. doi: 10.1186/s12969-022-00723-5. Pediatr Rheumatol Online J. 2022. PMID: 35927666 Free PMC article. Review.
-
Anti-MDA5 antibody-positive hypomyopathic dermatomyositis complicated with pneumomediastinum.Fukushima J Med Sci. 2018;64(2):89-94. doi: 10.5387/fms.2018-01. Fukushima J Med Sci. 2018. PMID: 30158335 Free PMC article.
-
Successful treatment of anti-melanoma differentiation-associated gene 5 antibody-positive dermatomyositis with rapidly progressive interstitial lung disease complicated by bilateral breast cancer following the additional tofacitinib: A case report.Mod Rheumatol Case Rep. 2025 Jan 16;9(1):93-99. doi: 10.1093/mrcr/rxae060. Mod Rheumatol Case Rep. 2025. PMID: 39330992
-
Successful treatment of anti-MDA5 antibody-positive refractory interstitial lung disease with plasma exchange therapy.Rheumatology (Oxford). 2020 Apr 1;59(4):767-771. doi: 10.1093/rheumatology/kez357. Rheumatology (Oxford). 2020. PMID: 31504956
Cited by
-
Clinical course and seroprevalence of COVID-19 in children with rheumatic diseases-cross-sectional study from a reference centre in Spain.Clin Rheumatol. 2022 Jun;41(6):1779-1784. doi: 10.1007/s10067-022-06186-z. Epub 2022 Apr 30. Clin Rheumatol. 2022. PMID: 35489011 Free PMC article.
-
Biologic drugs in the treatment of juvenile dermatomyositis: a literature review.Clin Rheumatol. 2024 Feb;43(2):591-602. doi: 10.1007/s10067-023-06740-3. Epub 2023 Aug 16. Clin Rheumatol. 2024. PMID: 37582998 Review.
-
Concurrent Infection with SARS-CoV-2 and Pneumocystis jirovecii in Immunocompromised and Immunocompetent Individuals.J Fungi (Basel). 2022 May 30;8(6):585. doi: 10.3390/jof8060585. J Fungi (Basel). 2022. PMID: 35736068 Free PMC article. Review.
-
Pneumocystis jirovecii Infections Among COVID-19 Patients: A Case Series and Literature Review.Open Forum Infect Dis. 2023 Jan 27;10(2):ofad043. doi: 10.1093/ofid/ofad043. eCollection 2023 Feb. Open Forum Infect Dis. 2023. PMID: 36817747 Free PMC article.
-
The role of SARS-CoV-2 immunosuppression and the therapy used to manage COVID-19 disease in the emergence of opportunistic fungal infections: A review.Curr Res Biotechnol. 2022;4:337-349. doi: 10.1016/j.crbiot.2022.08.001. Epub 2022 Aug 3. Curr Res Biotechnol. 2022. PMID: 35942223 Free PMC article. Review.
References
-
- Kurtzman DJB, Vleugels RA Anti-melanoma differentiation-associated gene 5 (MDA5) dermatomyositis: a concise review with an emphasis on distinctive clinical features. J Am Acad Dermatol. 2018;78(4):776–785. - PubMed
-
- Kobayashi I, Okura Y, Yamada M, et al. Anti-Melanoma differentiation-associated gene 5 antibody is a diagnostic and predictive marker for interstitial lung diseases associated with juvenile dermatomyositis. J Pediatr. 2011;158(4):675–677. - PubMed
-
- Kobayashi N, Takezaki S, Kobayashi I, et al. Clinical and laboratory features of fatal rapidly progressive interstitial lung disease associated with juvenile dermatomyositis. Rheumatology. 2015;54(5):784–791. - PubMed
-
- Le Goff B, Chérin P, Cantagrel A, et al. Pneumomediastinum in interstitial lung disease associated with dermatomyositis and polymyositis. Arthritis Rheum. 2009; 61(1):108–118. - PubMed
-
- Matsushita T, Mizumaki K, Kano M, et al. Antimelanoma differentiation-associated protein 5 antibody level is a novel tool for monitoring disease activity in rapidly progressive interstitial lung disease with dermatomyositis. Br J Dermatol. 2017;176(2):395–402. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
