

Antihypertensive therapies in moderate or severe aortic stenosis: a systematic review and meta-analysis
- PMID: 33020089
- PMCID: PMC7537451
- DOI: 10.1136/bmjopen-2020-036960
Antihypertensive therapies in moderate or severe aortic stenosis: a systematic review and meta-analysis
Abstract
Background: Hypertension confers a poor prognosis in moderate or severe aortic stenosis (AS), however, antihypertensive therapy (AHT) is often not prescribed due to the perceived deleterious effects of vasodilation and negative inotropes.
Objective: To assess the efficacy and safety outcomes of AHT in adults with moderate or severe AS.
Design: Systematic review and meta-analysis.
Data sources: The Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE and grey literature were searched without language restrictions up to 9 September 2019.
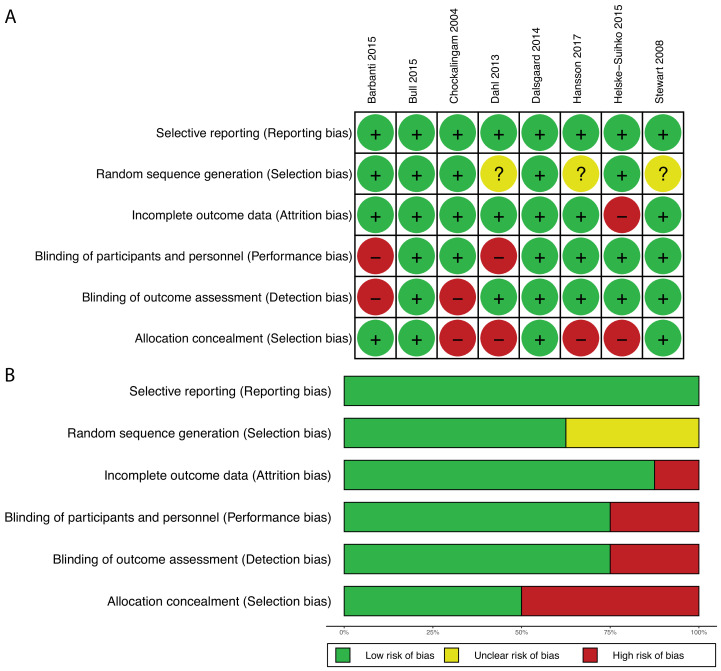
Study eligibility criteria, appraisal and synthesis methods: Two independent reviewers performed screening, data extraction and risk of bias assessments from a systematic search of observational studies and randomised controlled trials comparing AHT with a placebo or no AHT in adults with moderate or severe AS for any parameter of efficacy and safety outcomes. Conflicts were resolved by the third reviewer. Meta-analysis with pooled effect sizes using random-effects model, were estimated in R.
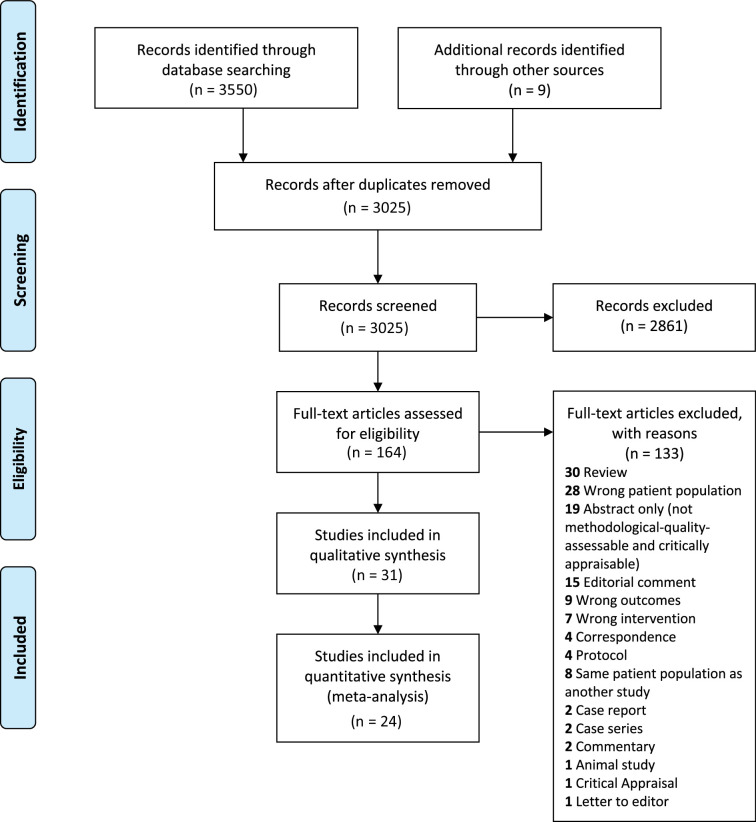
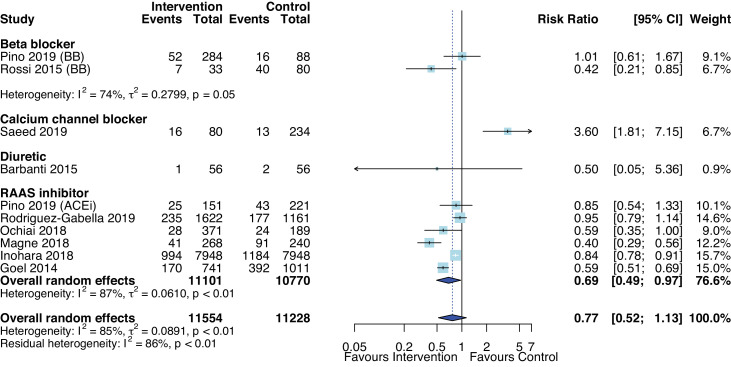
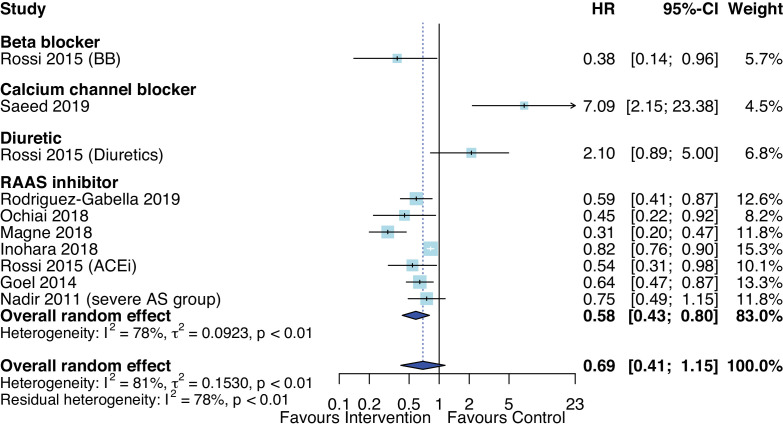
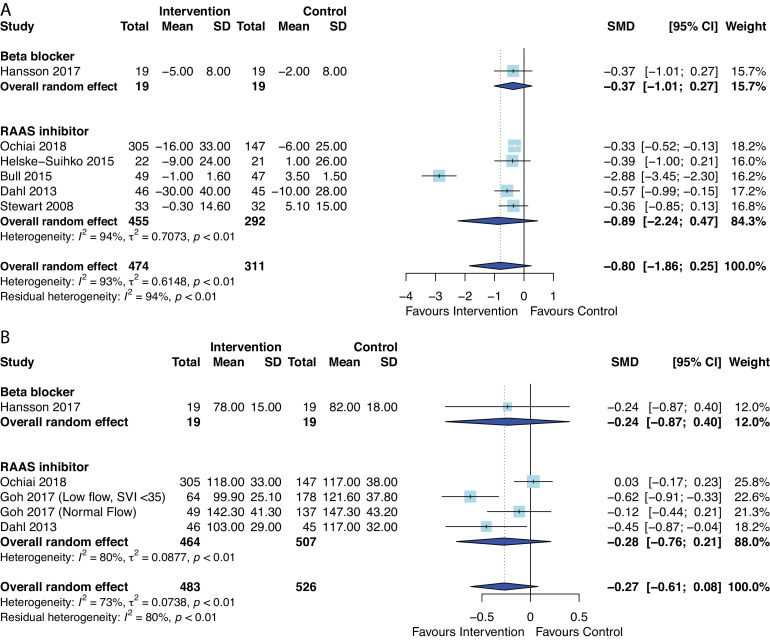
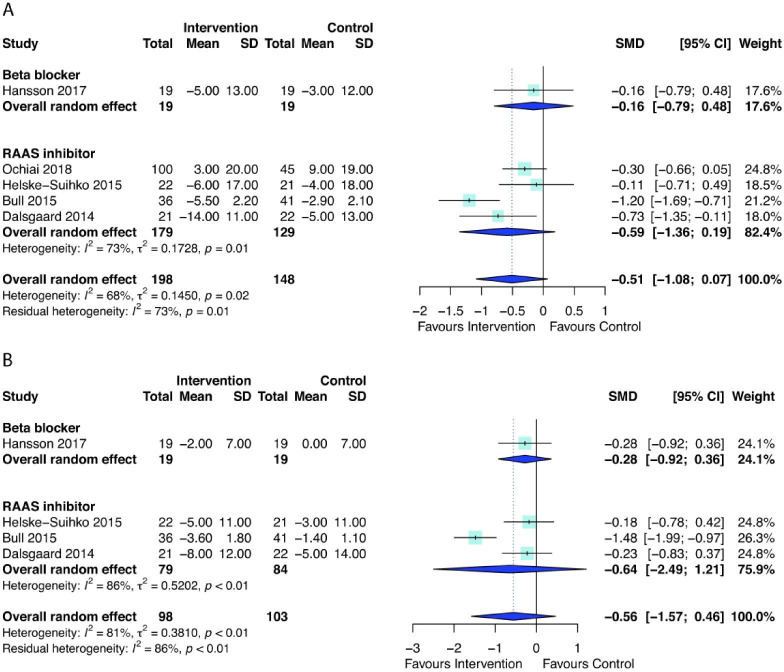
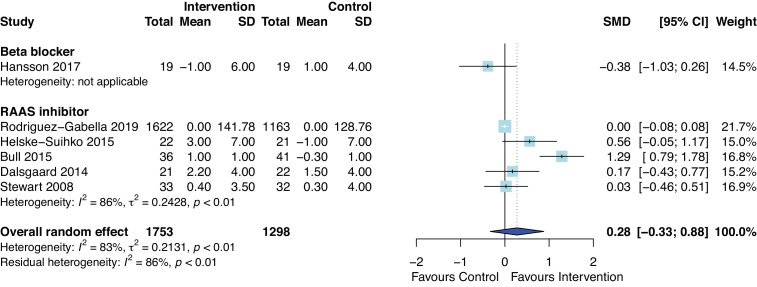
Main outcome measures: Mortality, Left Ventricular (LV) Mass Index, systolic blood pressure, diastolic blood pressure and LV ejection fraction RESULTS: From 3025 publications, 31 studies (26 500 patients) were included in the qualitative synthesis and 24 studies in the meta-analysis. AHT was not associated with mortality when all studies were pooled, but heterogeneity was substantial across studies. The effect size of AHT differed according to drug class. Renin-angiotensin-aldosterone system inhibitors (RAASi) were associated with reduced risk of mortality (Pooled HR 0.58, 95% CI 0.43 to 0.80, p=0.006), The differences in changes of haemodynamic or echocardiographic parameters from baseline with and without AHT did not reach statistical significance.
Conclusion: AHT appears safe, is well tolerated. RAASi were associated with clinical benefit in patients with moderate or severe AS.
Keywords: adult cardiology; hypertension; valvular heart disease.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from Australian Government Research Training Program (Research Scholarship) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Antihypertensive drug therapy for mild to moderate hypertension during pregnancy.Cochrane Database Syst Rev. 2018 Oct 1;10(10):CD002252. doi: 10.1002/14651858.CD002252.pub4. Cochrane Database Syst Rev. 2018. PMID: 30277556 Free PMC article.
-
Association Between Renin-Angiotensin-Aldosterone System Inhibitors and Clinical Outcomes in Patients With COVID-19: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Mar 1;4(3):e213594. doi: 10.1001/jamanetworkopen.2021.3594. JAMA Netw Open. 2021. PMID: 33787911 Free PMC article.
-
Calcium channel blockers for people with chronic kidney disease requiring dialysis.Cochrane Database Syst Rev. 2020 Oct 1;10(10):CD011064. doi: 10.1002/14651858.CD011064.pub2. Cochrane Database Syst Rev. 2020. PMID: 33000470 Free PMC article.
-
Blood pressure targets for the treatment of people with hypertension and cardiovascular disease.Cochrane Database Syst Rev. 2020 Sep 9;9(9):CD010315. doi: 10.1002/14651858.CD010315.pub4. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Nov 18;11:CD010315. doi: 10.1002/14651858.CD010315.pub5. PMID: 32905623 Free PMC article. Updated.
-
Blood pressure targets in adults with hypertension.Cochrane Database Syst Rev. 2020 Dec 17;12(12):CD004349. doi: 10.1002/14651858.CD004349.pub3. Cochrane Database Syst Rev. 2020. PMID: 33332584 Free PMC article.
Cited by
-
Systemic blood pressure in severe aortic stenosis: Haemodynamic correlates and long-term prognostic impact.ESC Heart Fail. 2023 Feb;10(1):274-283. doi: 10.1002/ehf2.14192. Epub 2022 Oct 7. ESC Heart Fail. 2023. PMID: 36205069 Free PMC article.
-
Arterial Hypertension in Aortic Valve Stenosis: A Critical Update.J Clin Med. 2021 Nov 26;10(23):5553. doi: 10.3390/jcm10235553. J Clin Med. 2021. PMID: 34884254 Free PMC article. Review.
-
Acute Heart Failure in an Almost-Centenarian Patient With Symptomatic Severe Aortic Stenosis Treated With Ivabradine.Cureus. 2022 Dec 2;14(12):e32142. doi: 10.7759/cureus.32142. eCollection 2022 Dec. Cureus. 2022. PMID: 36601174 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials