

Monitoring indirect impact of COVID-19 pandemic on services for cardiovascular diseases in the UK
- PMID: 33020224
- PMCID: PMC7536637
- DOI: 10.1136/heartjnl-2020-317870
Monitoring indirect impact of COVID-19 pandemic on services for cardiovascular diseases in the UK
Abstract
Objective: To monitor hospital activity for presentation, diagnosis and treatment of cardiovascular diseases during the COVID-19) pandemic to inform on indirect effects.
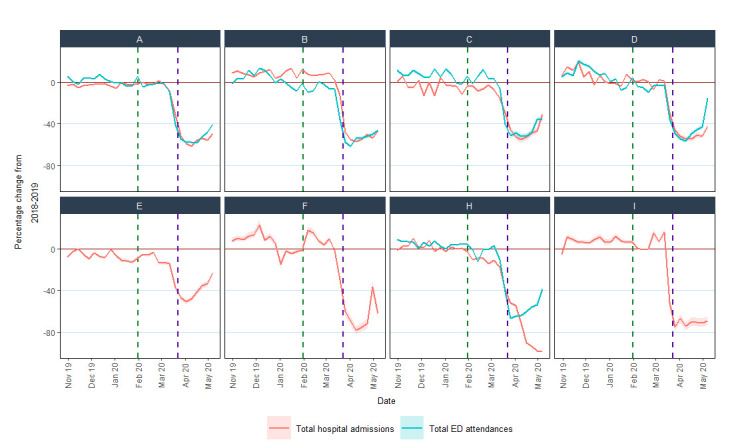
Methods: Retrospective serial cross-sectional study in nine UK hospitals using hospital activity data from 28 October 2019 (pre-COVID-19) to 10 May 2020 (pre-easing of lockdown) and for the same weeks during 2018-2019. We analysed aggregate data for selected cardiovascular diseases before and during the epidemic. We produced an online visualisation tool to enable near real-time monitoring of trends.
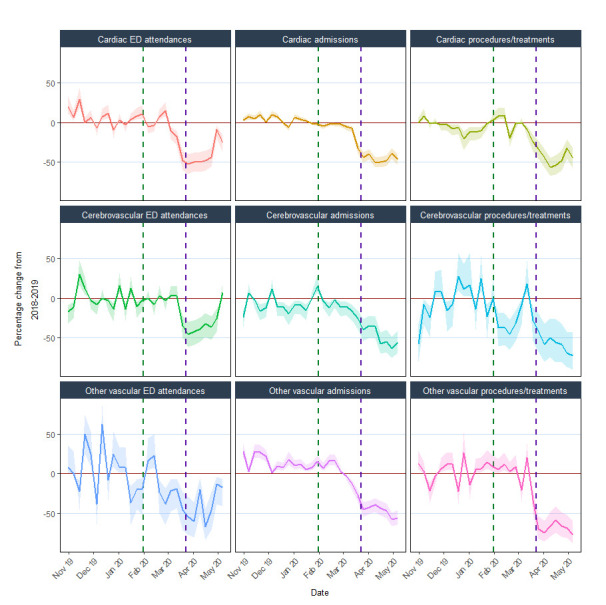
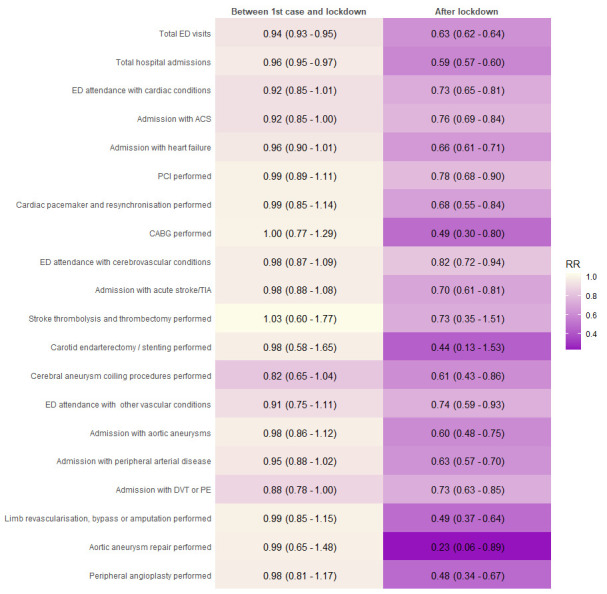
Results: Across nine hospitals, total admissions and emergency department (ED) attendances decreased after lockdown (23 March 2020) by 57.9% (57.1%-58.6%) and 52.9% (52.2%-53.5%), respectively, compared with the previous year. Activity for cardiac, cerebrovascular and other vascular conditions started to decline 1-2 weeks before lockdown and fell by 31%-88% after lockdown, with the greatest reductions observed for coronary artery bypass grafts, carotid endarterectomy, aortic aneurysm repair and peripheral arterial disease procedures. Compared with before the first UK COVID-19 (31 January 2020), activity declined across diseases and specialties between the first case and lockdown (total ED attendances relative reduction (RR) 0.94, 0.93-0.95; total hospital admissions RR 0.96, 0.95-0.97) and after lockdown (attendances RR 0.63, 0.62-0.64; admissions RR 0.59, 0.57-0.60). There was limited recovery towards usual levels of some activities from mid-April 2020.
Conclusions: Substantial reductions in total and cardiovascular activities are likely to contribute to a major burden of indirect effects of the pandemic, suggesting they should be monitored and mitigated urgently.
Keywords: aortic and arterial disease; epidemiology; global health care delivery; health care delivery; heart disease.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Comment in
-
Cardiovascular health and COVID-19: time to reinvent our systems and rethink our research priorities.Heart. 2020 Dec;106(24):1870-1872. doi: 10.1136/heartjnl-2020-318323. Epub 2020 Nov 3. Heart. 2020. PMID: 33144390 No abstract available.
-
Heartbeat: cardiovascular health in the time of COVID-19.Heart. 2020 Dec;106(24):1867-1869. doi: 10.1136/heartjnl-2020-318627. Heart. 2020. PMID: 33243784 No abstract available.
References
-
- James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. The Lancet 2018;392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous