

Posterior Stabilization Without Neural Decompression in Osteoporotic Thoracolumbar Fractures With Dynamic Cord Compression Causing Incomplete Neurological Deficits
- PMID: 33021093
- PMCID: PMC9121152
- DOI: 10.1177/2192568220956954
Posterior Stabilization Without Neural Decompression in Osteoporotic Thoracolumbar Fractures With Dynamic Cord Compression Causing Incomplete Neurological Deficits
Abstract
Study design: Prospective cohort study.
Objectives: Management of osteoporotic vertebral compression fracture (OVCF) remains an unsolved problem for a spine surgeon. We hypothesize that instability at the fracture site rather than neural compression is the main factor leading to a neurological deficit in patients with OVCF.
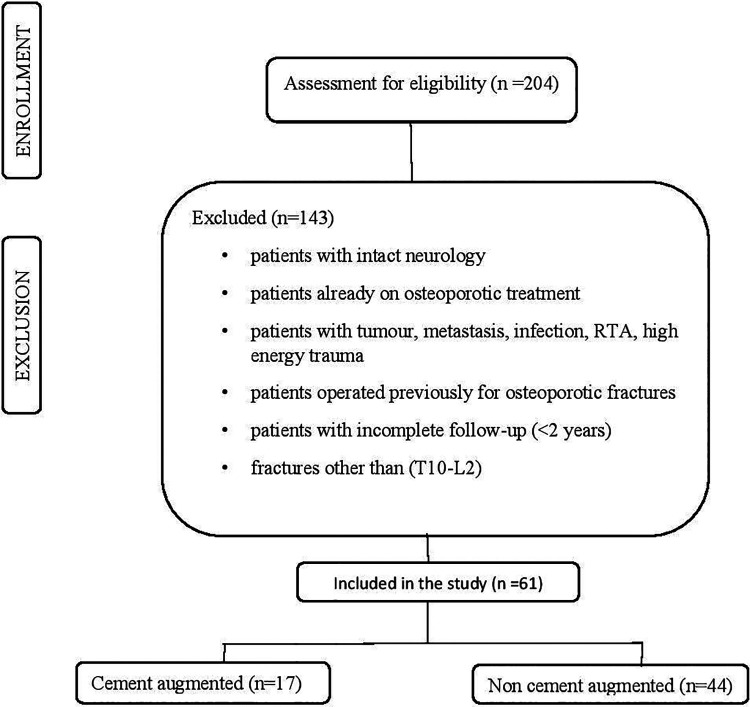
Methods: In this study, the prospective data of patients with osteoporotic fractures with incomplete neurological deficits from January 2015 to December 2017 was analyzed in those who underwent posterior instrumented fusion without neural decompression.
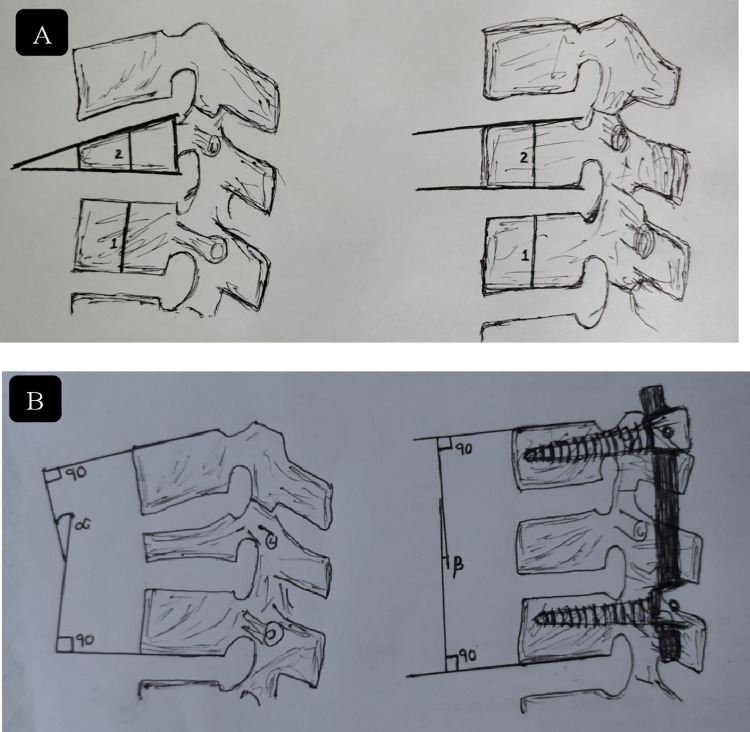
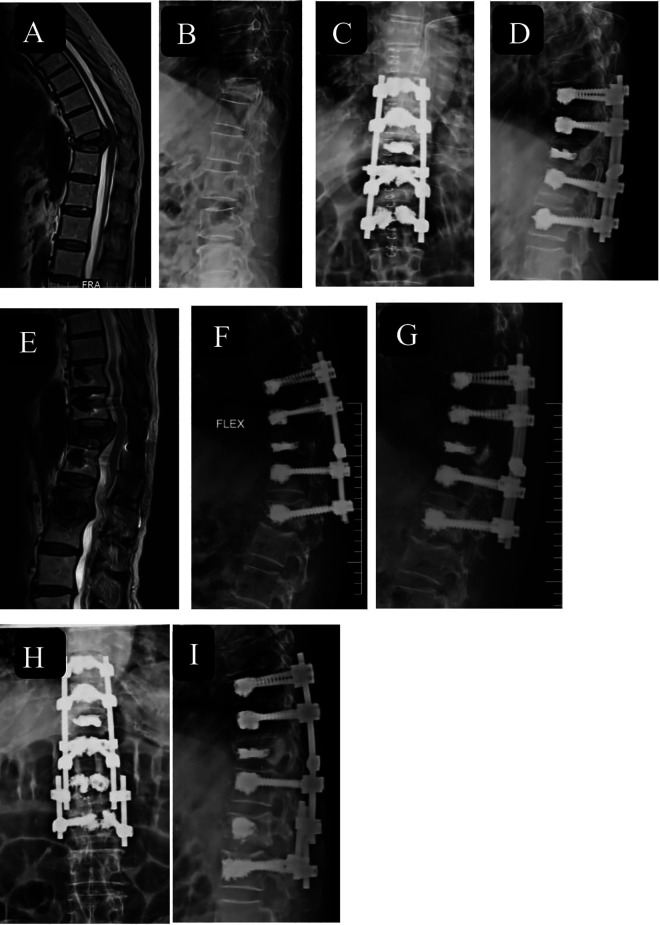
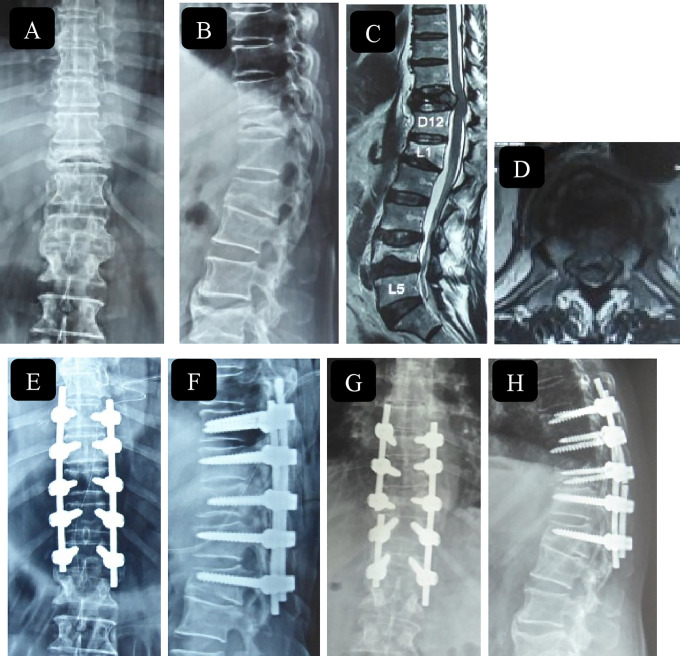
Results: A total of 61 patients received posterior indirect decompression via ligamentotaxis and stabilization only. Of these 17 patients had polymethylmethacrylate (PMMA) augmented screws and in 44 patients no PMMA augmentation was done. The mean preoperative kyphosis was 27.12° ± 9.63°, there was an improvement of 13.5° ± 6.87° in the immediate postoperative period and at the final follow-up, kyphosis was 13.7° ± 7.29° with a loss of correction by 2.85° ± 3.7°. The height restoration at the final follow-up was 45.4% ± 18.29%. In all patients, back pain was relieved, and neurological improvement was obtained by at least 1 American Spinal Injury Association Impairment Scale in all except 3 patients.
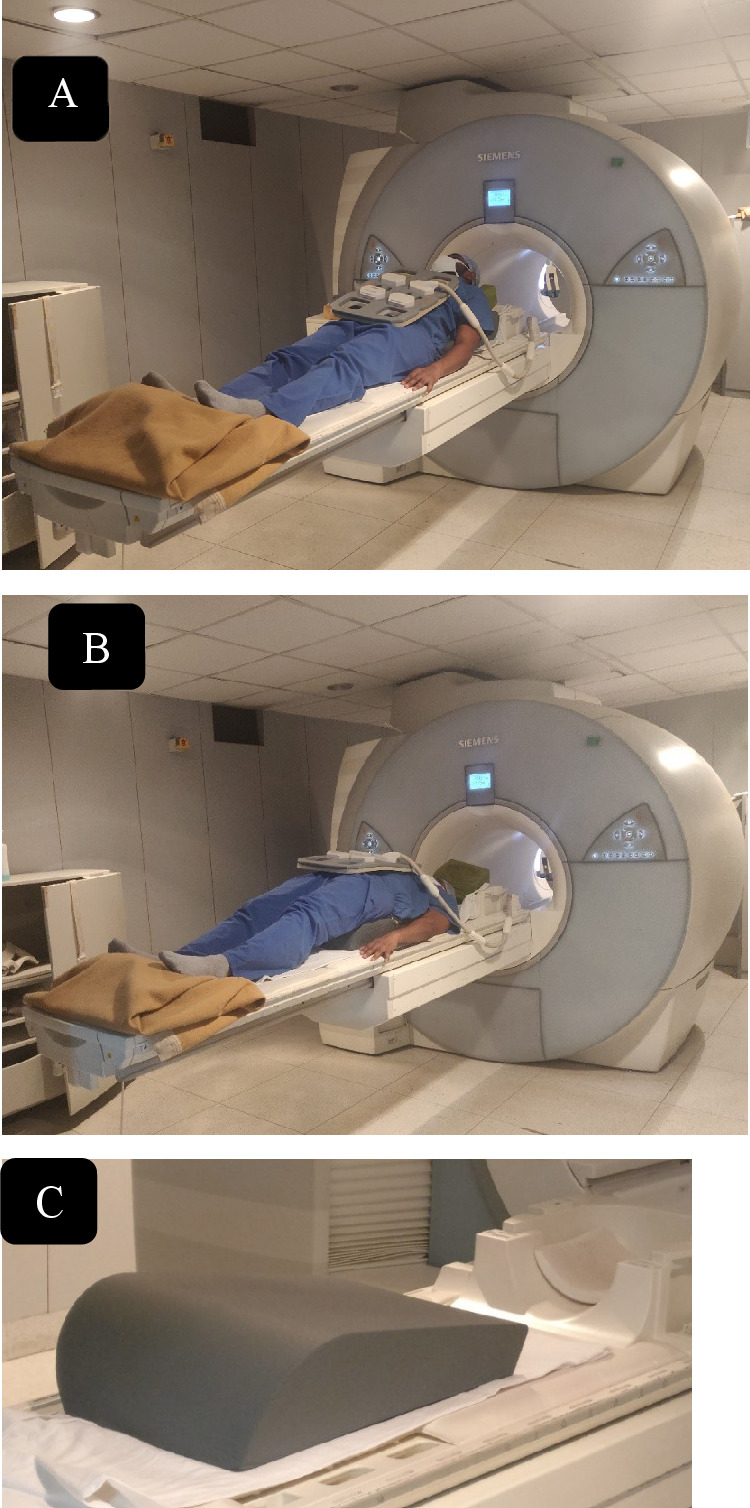
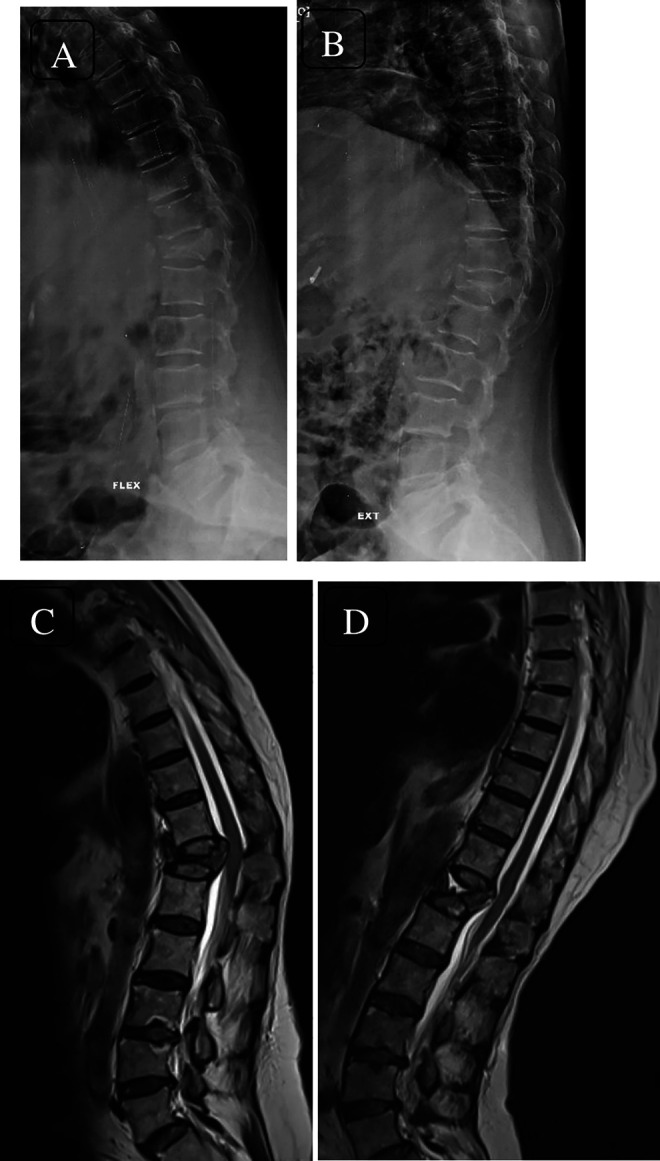
Conclusion: We propose that neural decompression of the spinal cord is not always necessary for the treatment of neurological impairment in patients with osteoporotic vertebral collapse with dynamic mobility. Dynamic magnetic resonance imaging is a valuable tool to make an accurate diagnosis and determine precise surgical plan and improving the surgical strategy of OVCF.
Keywords: neurological deficit; osteoporosis; thoracolumbar; vertebral compression fracture.
Conflict of interest statement
Figures

References
-
- Arciero RA, Leung KY, Pierce JH. Spontaneous unstable burst fracture of the thoracolumbar spine in osteoporosis. a report of two cases. Spine (Phila Pa 1976). 1989;14:114–117. doi:10.1097/00007632-198901000-00024 - PubMed
-
- Tanaka S, Kubota M, Fujimoto Y, Hayashi J, Nishikawa K. Conus medullaris syndrome secondary to an L1 burst fracture in osteoporosis: a case report. Spine (Phila Pa 1976). 1993;18:2131–2134. doi:10.1097/00007632-199310001-00034 - PubMed
-
- Chang KW, Chen YY, Lin CC, Hsu HL, Pai KC. Apical lordosating osteotomy and minimal segment fixation for the treatment of thoracic or thoracolumbar osteoporotic kyphosis. Spine (Phila Pa 1976). 2005;30:1674–1681. doi:10.1097/01.brs.0000170450.77554.bc - PubMed
-
- Kaneda K, Asano S, Hashimoto T, Satoh S, Fujiya M. The treatment of osteoporotic-posttraumatic vertebral collapse using the kaneda device and a bioactive ceramic vertebral prosthesis. Spine (Phila Pa 1976). 1992;17(8 suppl):S295–S303. doi:10.1097/00007632-199208001-00015 - PubMed
-
- Mochida J, Toh E, Chiba M, Nishimura K. Treatment of osteoporotic late collapse of a vertebral body of thoracic and lumbar spine. J Spinal Disord. 2001;14:393–398. doi:10.1097/00002517-200110000-00004 - PubMed
LinkOut - more resources
Full Text Sources
