

Midwifery continuity of care versus standard maternity care for women at increased risk of preterm birth: A hybrid implementation-effectiveness, randomised controlled pilot trial in the UK
- PMID: 33022010
- PMCID: PMC7537886
- DOI: 10.1371/journal.pmed.1003350
Midwifery continuity of care versus standard maternity care for women at increased risk of preterm birth: A hybrid implementation-effectiveness, randomised controlled pilot trial in the UK
Abstract
Background: Midwifery continuity of care is the only health system intervention shown to reduce preterm birth (PTB) and improve perinatal survival, but no trial evidence exists for women with identified risk factors for PTB. We aimed to assess feasibility, fidelity, and clinical outcomes of a model of midwifery continuity of care linked with a specialist obstetric clinic for women considered at increased risk for PTB.
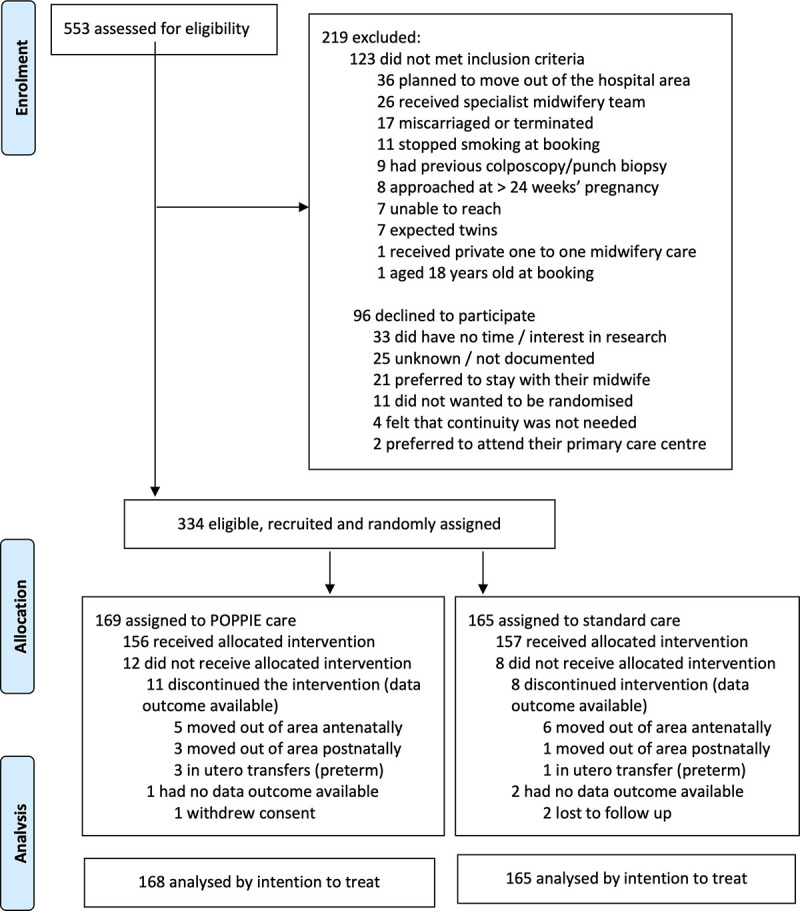
Methods and findings: We conducted a hybrid implementation-effectiveness, randomised, controlled, unblinded, parallel-group pilot trial at an inner-city maternity service in London (UK), in which pregnant women identified at increased risk of PTB were randomly assigned (1:1) to either midwifery continuity of antenatal, intrapartum, and postnatal care (Pilot study Of midwifery Practice in Preterm birth Including women's Experiences [POPPIE] group) or standard care group (maternity care by different midwives working in designated clinical areas). Pregnant women attending for antenatal care at less than 24 weeks' gestation were eligible if they fulfilled one or more of the following criteria: previous cervical surgery, cerclage, premature rupture of membranes, PTB, or late miscarriage; previous short cervix or short cervix this pregnancy; or uterine abnormality and/or current smoker of tobacco. Feasibility outcomes included eligibility, recruitment and attrition rates, and fidelity of the model. The primary outcome was a composite of appropriate and timely interventions for the prevention and/or management of preterm labour and birth. We analysed by intention to treat. Between 9 May 2017 and 30 September 2018, 334 women were recruited; 169 women were allocated to the POPPIE group and 165 to the standard group. Mean maternal age was 31 years; 32% of the women were from Black, Asian, and ethnic minority groups; 70% were in employment; and 46% had a university degree. Nearly 70% of women lived in areas of social deprivation. More than a quarter of women had at least one pre-existing medical condition and multiple risk factors for PTB. More than 75% of antenatal and postnatal visits were provided by a named/partner midwife, and a midwife from the POPPIE team was present at 80% of births. The incidence of the primary composite outcome showed no statistically significant difference between groups (POPPIE group 83.3% versus standard group 84.7%; risk ratio 0.98 [95% confidence interval (CI) 0.90 to 1.08]; p = 0.742). Infants in the POPPIE group were significantly more likely to have skin-to-skin contact after birth, to have it for a longer time, and to breastfeed immediately after birth and at hospital discharge. There were no differences in other secondary outcomes. The number of serious adverse events was similar in both groups and unrelated to the intervention (POPPIE group 6 versus standard group 5). Limitations of this study included the limited power and the nonmasking of group allocation; however, study assignment was masked to the statistician and researchers who analysed the data.
Conclusions: In this study, we found that it is feasible to set up and achieve fidelity of a model of midwifery continuity of care linked with specialist obstetric care for women at increased risk of PTB in an inner-city maternity service in London (UK), but there is no impact on most outcomes for this population group. Larger appropriately powered trials are needed, including in other settings, to evaluate the impact of relational continuity and hypothesised mechanisms of effect based on increased trust and engagement, improved care coordination, and earlier referral on disadvantaged communities, including women with complex social factors and social vulnerability.
Trial registration: We prospectively registered the pilot trial on the UK Clinical Research Network Portfolio Database (ID number: 31951, 24 April 2017). We registered the trial on the International Standard Randomised Controlled Trial Number (ISRCTN) (Number: 37733900, 21 August 2017) and before trial recruitment was completed (30 September 2018) when informed that prospective registration for a pilot trial was also required in a primary clinical trial registry recognised by WHO and the International Committee of Medical Journal Editors (ICMJE). The protocol as registered and published has remained unchanged, and the analysis conforms to the original plan.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RT reports support from Mirvie and Vidya Health Limited outside the submitted work. AHS reports grants from Hologic outside the submitted work. PTS is partly funded by Tommy’s and NIHR ARC South London. CFT, DB, ALB, MB, KC, PC, SAS, CS, and PTS declare no competing interests.
Figures
References
-
- WHO: recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths, Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet Gynecol Scand. 1977;56: 247–253. - PubMed
-
- World Health Organization. Born Too Soon: The Global Action Report On Preterm Birth. Geneva, Switzerland: WHO; 2012.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
