

Association between prehospital time and outcome of trauma patients in 4 Asian countries: A cross-national, multicenter cohort study
- PMID: 33022018
- PMCID: PMC7537901
- DOI: 10.1371/journal.pmed.1003360
Association between prehospital time and outcome of trauma patients in 4 Asian countries: A cross-national, multicenter cohort study
Abstract
Background: Whether rapid transportation can benefit patients with trauma remains controversial. We determined the association between prehospital time and outcome to explore the concept of the "golden hour" for injured patients.
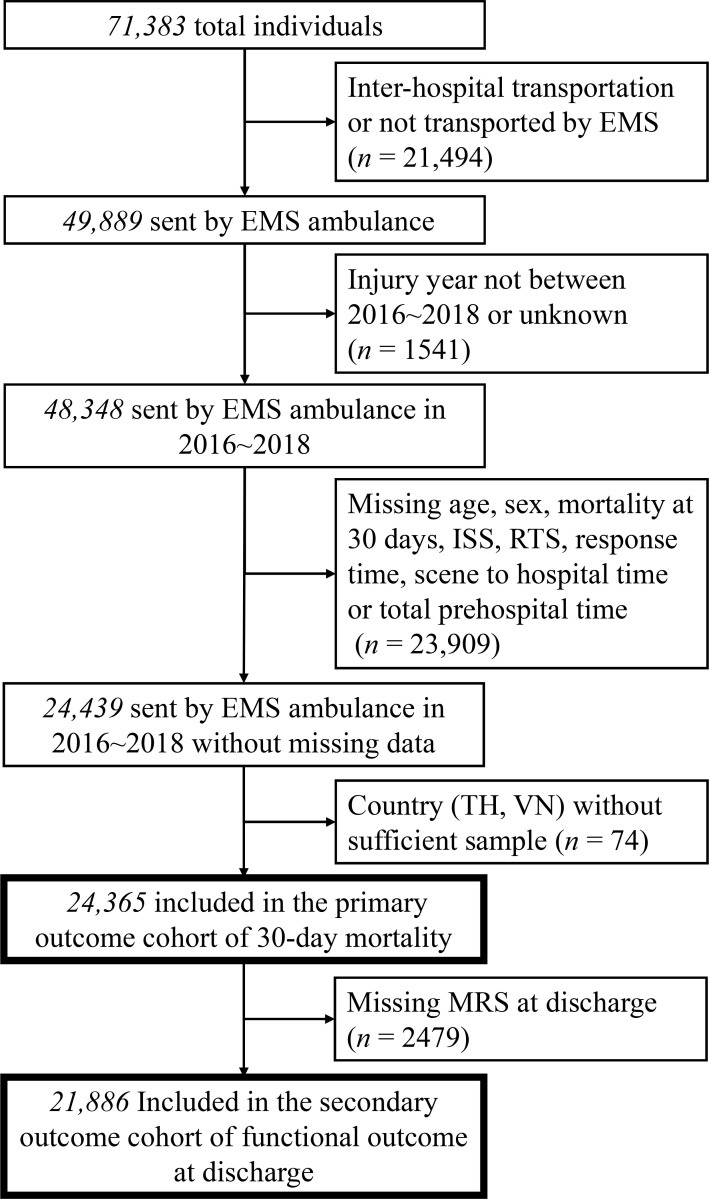
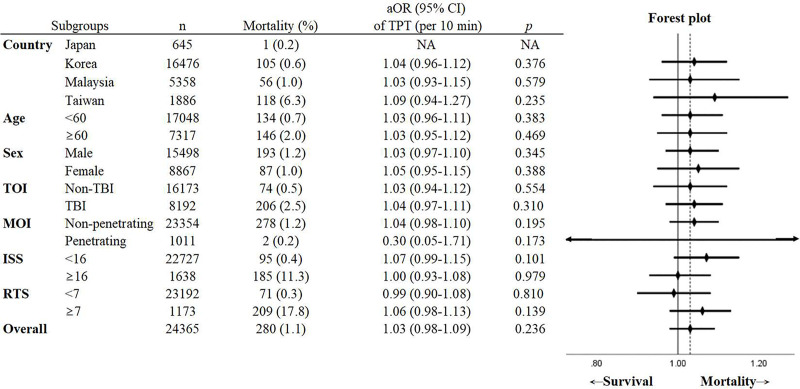
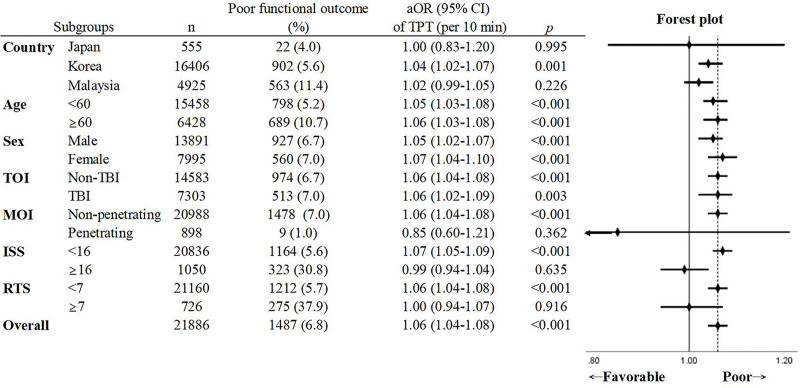
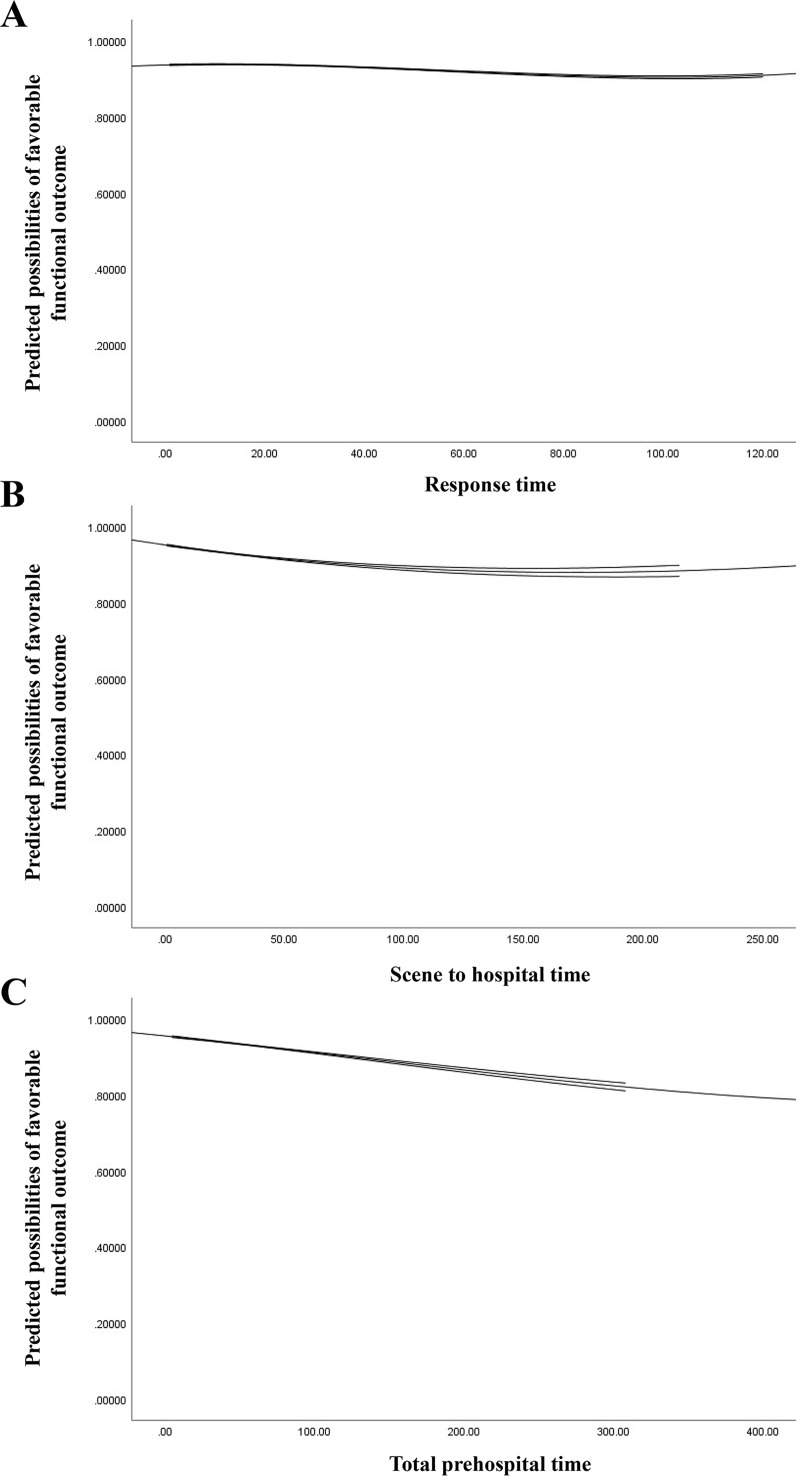
Methods and findings: We conducted a retrospective cohort study of trauma patients transported from the scene to hospitals by emergency medical service (EMS) from January 1, 2016, to November 30, 2018, using data from the Pan-Asia Trauma Outcomes Study (PATOS) database. Prehospital time intervals were categorized into response time (RT), scene to hospital time (SH), and total prehospital time (TPT). The outcomes were 30-day mortality and functional status at hospital discharge. Multivariable logistic regression was used to investigate the association of prehospital time and outcomes to adjust for factors including age, sex, mechanism and type of injury, Injury Severity Score (ISS), Revised Trauma Score (RTS), and prehospital interventions. Overall, 24,365 patients from 4 countries (645 patients from Japan, 16,476 patients from Korea, 5,358 patients from Malaysia, and 1,886 patients from Taiwan) were included in the analysis. Among included patients, the median age was 45 years (lower quartile [Q1]-upper quartile [Q3]: 25-62), and 15,498 (63.6%) patients were male. Median (Q1-Q3) RT, SH, and TPT were 20 (Q1-Q3: 12-39), 21 (Q1-Q3: 16-29), and 47 (Q1-Q3: 32-60) minutes, respectively. In all, 280 patients (1.1%) died within 30 days after injury. Prehospital time intervals were not associated with 30-day mortality. The adjusted odds ratios (aORs) per 10 minutes of RT, SH, and TPT were 0.99 (95% CI 0.92-1.06, p = 0.740), 1.08 (95% CI 1.00-1.17, p = 0.065), and 1.03 (95% CI 0.98-1.09, p = 0.236), respectively. However, long prehospital time was detrimental to functional survival. The aORs of RT, SH, and TPT per 10-minute delay were 1.06 (95% CI 1.04-1.08, p < 0.001), 1.05 (95% CI 1.01-1.08, p = 0.007), and 1.06 (95% CI 1.04-1.08, p < 0.001), respectively. The key limitation of our study is the missing data inherent to the retrospective design. Another major limitation is the aggregate nature of the data from different countries and unaccounted confounders such as in-hospital management.
Conclusions: Longer prehospital time was not associated with an increased risk of 30-day mortality, but it may be associated with increased risk of poor functional outcomes in injured patients. This finding supports the concept of the "golden hour" for trauma patients during prehospital care in the countries studied.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Prehospital times and outcomes of patients who had hypotension at the scene after trauma: A nationwide multicentre retrospective study.Injury. 2020 May;51(5):1224-1230. doi: 10.1016/j.injury.2020.02.002. Epub 2020 Feb 5. Injury. 2020. PMID: 32057459
-
Prehospital Time Following Traumatic Injury Is Independently Associated With the Need for In-Hospital Blood and Early Mortality for Specific Injury Types.Air Med J. 2024 Jan-Feb;43(1):47-54. doi: 10.1016/j.amj.2023.09.013. Epub 2023 Nov 28. Air Med J. 2024. PMID: 38154840
-
Prehospital Intervals and In-Hospital Trauma Mortality: A Retrospective Study from a Level I Trauma Center.Prehosp Disaster Med. 2020 Oct;35(5):508-515. doi: 10.1017/S1049023X20000904. Epub 2020 Jul 17. Prehosp Disaster Med. 2020. PMID: 32674744
-
Outcomes of Pediatric Patients in Secondary Transport to Tertiary Hospital: A Retrospective Observational Study.Pediatr Emerg Care. 2022 Jun 1;38(6):283-289. doi: 10.1097/PEC.0000000000002711. Epub 2022 Apr 18. Pediatr Emerg Care. 2022. PMID: 35436767 Review.
-
The effect of transfer status on trauma outcomes in low- and middle-income countries: A systematic review and meta-analysis.Injury. 2022 Mar;53(3):885-894. doi: 10.1016/j.injury.2021.10.010. Epub 2021 Oct 13. Injury. 2022. PMID: 34689985 Free PMC article.
Cited by
-
Shock index, modified shock index, age shock index score, and reverse shock index multiplied by Glasgow Coma Scale predicting clinical outcomes in traumatic brain injury: Evidence from a 10-year analysis in a single center.Front Med (Lausanne). 2022 Nov 22;9:999481. doi: 10.3389/fmed.2022.999481. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36482909 Free PMC article.
-
Outcomes of blunt trauma patients in police versus ground ambulance transport across US trauma centers.Acute Med Surg. 2025 May 8;12(1):e70061. doi: 10.1002/ams2.70061. eCollection 2025 Jan-Dec. Acute Med Surg. 2025. PMID: 40353044 Free PMC article.
-
The effect of a new in-hospital trauma care model on the outcomes of severely injured trauma patients in the emergency department: a retrospective observational study in China.BMC Emerg Med. 2025 Mar 24;25(1):47. doi: 10.1186/s12873-025-01203-1. BMC Emerg Med. 2025. PMID: 40128673 Free PMC article.
-
Epidemiology of patients assessed for trauma by Swedish ambulance services: a retrospective registry study.BMC Emerg Med. 2024 Jan 8;24(1):11. doi: 10.1186/s12873-023-00924-5. BMC Emerg Med. 2024. PMID: 38191306 Free PMC article.
-
Influence of on-scene time and prehospital interventions on inhospital mortality in trauma patients.BMC Emerg Med. 2025 Aug 20;25(1):163. doi: 10.1186/s12873-025-01324-7. BMC Emerg Med. 2025. PMID: 40830842 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
