

Targeting acute kidney injury in COVID-19
- PMID: 33022712
- PMCID: PMC7665651
- DOI: 10.1093/ndt/gfaa231
Targeting acute kidney injury in COVID-19
Abstract
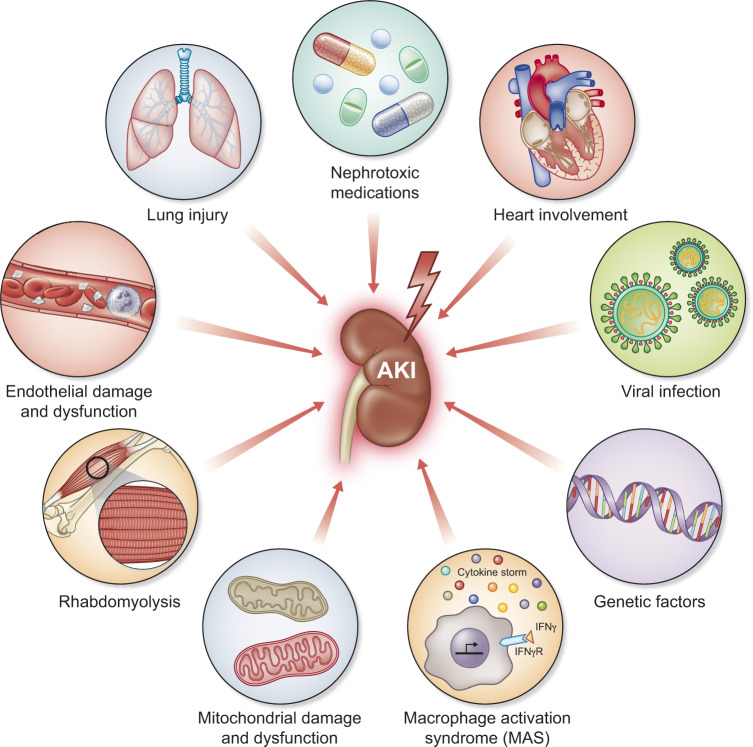
As of 15 August 2020, Coronavirus disease 2019 (COVID-19) has been reported in >21 million people world-wide and is responsible for more than 750,000 deaths. The occurrence of acute kidney injury (AKI) in patients hospitalized with COVID-19 has been reported to be as high as 43%. This is comparable to AKI in other forms of pneumonia requiring hospitalization, as well as in non-infectious conditions like cardiac surgery. The impact of AKI on COVID-19 outcomes is difficult to assess at present but, similar to other forms of sepsis, AKI is strongly associated with hospital mortality. Indeed, mortality is reported to be very low in COVID-19 patients without AKI. Given that AKI contributes to fluid and acid-base imbalances, compromises immune response and may impair resolution of inflammation, it seems likely that AKI contributes to mortality in these patients. The pathophysiologic mechanisms of AKI in COVID-19 are thought to be multifactorial including systemic immune and inflammatory responses induced by viral infection, systemic tissue hypoxia, reduced renal perfusion, endothelial damage and direct epithelial infection with Severe Acute Respiratory Syndrome Coronavirus 2. Mitochondria play a central role in the metabolic deregulation in the adaptive response to the systemic inflammation and are also found to be vital in response to both direct viral damage and tissue reperfusion. These stress conditions are associated with increased glycolysis and reduced fatty acid oxidation. Thus, there is a strong rationale to target AKI for therapy in COVID-19. Furthermore, many approaches that have been developed for other etiologies of AKI such as sepsis, inflammation and ischemia-reperfusion, have relevance in the treatment of COVID-19 AKI and could be rapidly pivoted to this new disease.
Keywords: AKI; COVID-19; mitochondria; mortality; sepsis.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Figures
Similar articles
-
Acute Kidney Injury in COVID-19 Patients: An Inner City Hospital Experience and Policy Implications.Am J Nephrol. 2020;51(10):786-796. doi: 10.1159/000511160. Epub 2020 Oct 2. Am J Nephrol. 2020. PMID: 33011717 Free PMC article.
-
Clinical Characteristics and Outcomes of Community- and Hospital-Acquired Acute Kidney Injury with COVID-19 in a US Inner City Hospital System.Cardiorenal Med. 2020;10(4):223-231. doi: 10.1159/000509182. Epub 2020 Jun 18. Cardiorenal Med. 2020. PMID: 32554965 Free PMC article.
-
COVID-19 and Kidney Disease: Update on Epidemiology, Clinical Manifestations, Pathophysiology and Management.J Coll Physicians Surg Pak. 2020 Jun;30(6):19-25. doi: 10.29271/jcpsp.2020.Supp1.S19. J Coll Physicians Surg Pak. 2020. PMID: 32723443
-
Acute kidney injury in critically ill patients with COVID-19.Intensive Care Med. 2020 Jul;46(7):1339-1348. doi: 10.1007/s00134-020-06153-9. Epub 2020 Jun 12. Intensive Care Med. 2020. PMID: 32533197 Free PMC article. Review.
-
Renal changes and acute kidney injury in covid-19: a systematic review.Rev Assoc Med Bras (1992). 2020 Sep 21;66Suppl 2(Suppl 2):112-117. doi: 10.1590/1806-9282.66.S2.112. eCollection 2020. Rev Assoc Med Bras (1992). 2020. PMID: 32965368
Cited by
-
The prognostic value of prognostic nutritional index and renal function indicators for mortality prediction in severe COVID-19 elderly patients: A retrospective study.Medicine (Baltimore). 2024 May 17;103(20):e38213. doi: 10.1097/MD.0000000000038213. Medicine (Baltimore). 2024. PMID: 38758852 Free PMC article.
-
Pathophysiological, immunological, and inflammatory features of long COVID.Front Immunol. 2024 Feb 28;15:1341600. doi: 10.3389/fimmu.2024.1341600. eCollection 2024. Front Immunol. 2024. PMID: 38482000 Free PMC article. Review.
-
Calcineurin inhibitors and related medicines: a cohort study examining England's primary care prescription changes during the COVID-19 pandemic (January 2019 to March 2021).Daru. 2022 Jun;30(1):59-66. doi: 10.1007/s40199-021-00431-7. Epub 2022 Jan 24. Daru. 2022. PMID: 35075618 Free PMC article.
-
Can Biomarkers Predict Kidney Function Recovery and Mortality in Patients with Critical COVID-19 and Acute Kidney Injury?Diagnostics (Basel). 2025 Aug 5;15(15):1960. doi: 10.3390/diagnostics15151960. Diagnostics (Basel). 2025. PMID: 40804924 Free PMC article.
-
Acute Kidney Injury and Urinary and Histopathological Disorders in Kidney Transplant Patients with SARS-CoV-2 Infection.Transplant Proc. 2022 Jul-Aug;54(6):1471-1475. doi: 10.1016/j.transproceed.2022.04.008. Epub 2022 Apr 11. Transplant Proc. 2022. PMID: 35649967 Free PMC article.
References
-
- Chan L, Chaudhary K, Saha A. et al. Acute kidney injury in hospitalized patients with COVID-19. medRxiv 2020. doi:10.1101/2020.05.04.20090944
-
- Kellum JA, Prowle JR.. Paradigms of acute kidney injury in the intensive care setting. Nat Rev Nephrol 2018; 14: 217–230 - PubMed
-
- Ren X, Glende J, Al-Falah M. et al. Analysis of ACE2 in polarized epithelial cells: surface expression and function as receptor for severe acute respiratory syndrome-associated coronavirus. J Gen Virol 2006; 87: 1691–1695 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
