

Clinical and cardiac characteristics of COVID-19 mortalities in a diverse New York City Cohort
- PMID: 33022765
- PMCID: PMC7675758
- DOI: 10.1111/jce.14772
Clinical and cardiac characteristics of COVID-19 mortalities in a diverse New York City Cohort
Abstract
Introduction: Electrocardiographic characteristics in COVID-19-related mortality have not yet been reported, particularly in racial/ethnic minorities.
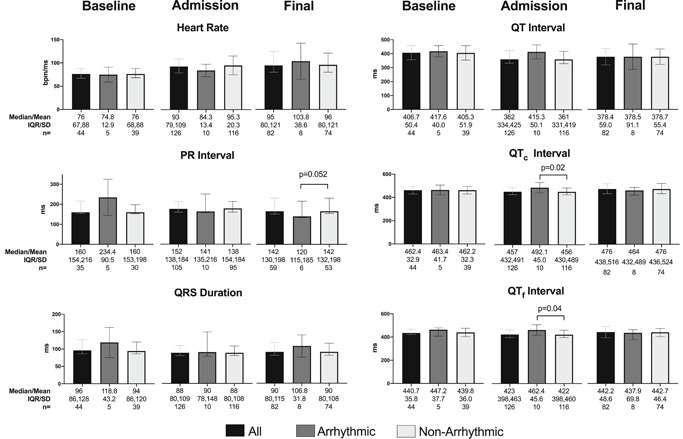
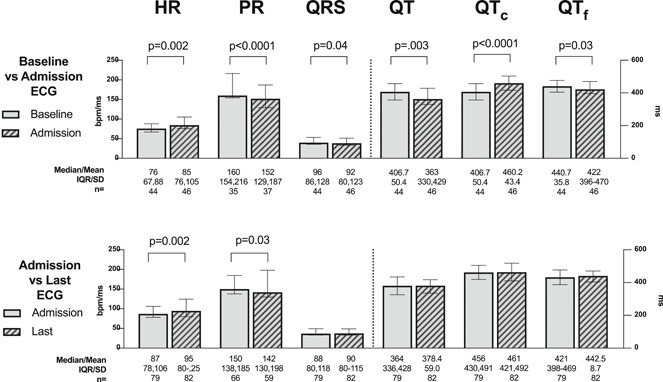
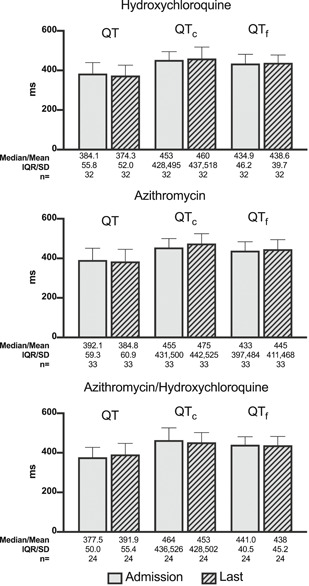
Methods and results: We reviewed demographics, laboratory and cardiac tests, medications, and cardiac rhythm proximate to death or initiation of comfort care for patients hospitalized with a positive SARS-CoV-2 reverse-transcriptase polymerase chain reaction in three New York City hospitals between March 1 and April 3, 2020 who died. We described clinical characteristics and compared factors contributing toward arrhythmic versus nonarrhythmic death. Of 1258 patients screened, 133 died and were enrolled. Of these, 55.6% (74/133) were male, 69.9% (93/133) were racial/ethnic minorities, and 88.0% (117/133) had cardiovascular disease. The last cardiac rhythm recorded was VT or fibrillation in 5.3% (7/133), pulseless electrical activity in 7.5% (10/133), unspecified bradycardia in 0.8% (1/133), and asystole in 26.3% (35/133). Most 74.4% (99/133) died receiving comfort measures only. The most common abnormalities on admission electrocardiogram included abnormal QRS axis (25.8%), atrial fibrillation/flutter (14.3%), atrial ectopy (12.0%), and right bundle branch block (11.9%). During hospitalization, an additional 17.6% developed atrial ectopy, 14.7% ventricular ectopy, 10.1% atrial fibrillation/flutter, and 7.8% a right ventricular abnormality. Arrhythmic death was confirmed or suspected in 8.3% (11/133) associated with age, coronary artery disease, asthma, vasopressor use, longer admission corrected QT interval, and left bundle branch block (LBBB).
Conclusions: Conduction, rhythm, and electrocardiographic abnormalities were common during COVID-19-related hospitalization. Arrhythmic death was associated with age, coronary artery disease, asthma, longer admission corrected QT interval, LBBB, ventricular ectopy, and usage of vasopressors. Most died receiving comfort measures.
Keywords: COVID-19; arrhythmia; cardiac death; electrocardiography; epidemiology; sudden death.
© 2020 Wiley Periodicals LLC.
Figures
References
-
- COVID‐19 Data ; 2020. https://www1.nyc.gov/site/doh/covid/covid-19-data.page. Accessed May 28, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
