

The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy
- PMID: 33023215
- PMCID: PMC7601888
- DOI: 10.3390/diagnostics10100780
The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy
Abstract
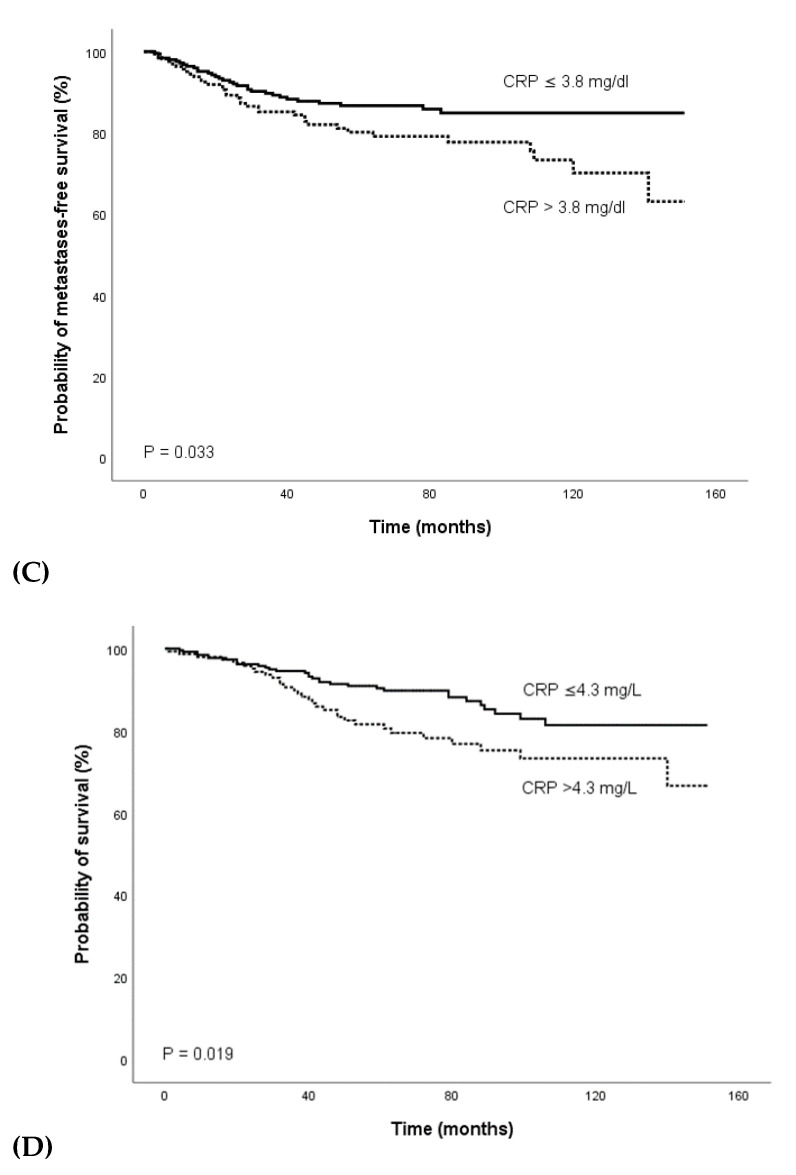
The aim of the present study was to investigate the association of the pre-treatment C-reactive protein (CRP) plasma level with survival outcomes in a cohort of 423 consecutive patients with locally advanced rectal cancer treated with neo-adjuvant radiochemotherapy followed by surgical resection. To evaluate the prognostic value of the CRP level for clinical endpoints recurrence-free survival (RFS), local-regional control (LC), metastases-free survival (MFS), and overall survival (OS), uni- and multivariate Cox regression analyses were applied, and survival rates were calculated using Kaplan-Meier analysis. The median follow-up time was 73 months. In univariate analyses, the pre-treatment CRP level was a significant predictor of RFS (hazard ratio (HR) 1.015, 95% CI 1.006-1.023; p < 0.001), LC (HR 1.015, 95% CI 1.004-1.027; p = 0.009), MFS (HR 1.014, 95% CI 1.004-1.023; p = 0.004), and OS (HR 1.016, 95% CI 1.007-1.024; p < 0.001). Additionally, univariate analysis identified the MRI circumferential resection margin (mrCRM) and pre-treatment carcinoembryonic antigen (CEA) as significant predictor of RFS (HR 2.082, 95% CI 1.106-3.919; p = 0.023 and HR 1.005, 95% CI 1.002-1.008; p < 0.001). Univariate analysis also revealed a significant association of the mrCRM (HR 2.089, 95% CI 1.052-4.147; p = 0.035) and CEA (HR 1.006, 95% CI 1.003-1.008; p < 0.001) with MFS. Age and CEA were prognostic factors for OS (HR 1.039, 95% CI 1.013-1.066; p = 0.003 and HR 1.005, 95% CI 1.002-1.008; p < 0.001). In multivariate analysis that included parameters with a p-level < 0.20 in univariate analysis, the pre-treatment CRP remained a significant prognostic factor for RFS (HR 1.013, 95%CI 1.001-1.025; p = 0.036), LC (HR 1.014, 95% CI 1.001-1.027; p = 0.031), and MFS (HR 1.013, 95% CI 1.000-1.027; p = 0.046). The results support the hypothesis that an elevated pre-treatment CRP level is a predictor of poor outcome. If confirmed by additional studies, this easily measurable biomarker could contribute to the identification of patients who might be candidates for more aggressive local or systemic treatment approaches or the administration of anti-inflammatory drugs.
Keywords: C-reactive protein (CRP); biomarker; inflammation; locally advanced rectal cancer; neo-adjuvant radiochemotherapy; outcome; prognostic factor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer.Diagnostics (Basel). 2023 Feb 11;13(4):679. doi: 10.3390/diagnostics13040679. Diagnostics (Basel). 2023. PMID: 36832166 Free PMC article.
-
The Pre-Treatment C-Reactive Protein Represents a Prognostic Factor in Patients with Oral and Oropharyngeal Cancer Treated with Radiotherapy.Cancers (Basel). 2020 Mar 8;12(3):626. doi: 10.3390/cancers12030626. Cancers (Basel). 2020. PMID: 32182693 Free PMC article.
-
Prognostic value of CEA and CA19-9 in patients with local advanced rectal cancer receiving neoadjuvant chemoradiotherapy, radical surgery and postoperative chemotherapy.Transl Cancer Res. 2021 Jan;10(1):88-98. doi: 10.21037/tcr-20-2269. Transl Cancer Res. 2021. PMID: 35116242 Free PMC article.
-
The elevated C-reactive protein level is associated with poor prognosis in prostate cancer patients treated with radiotherapy.Eur J Cancer. 2015 Mar;51(5):610-9. doi: 10.1016/j.ejca.2015.01.002. Epub 2015 Jan 21. Eur J Cancer. 2015. PMID: 25618827
-
Prognostic role of elevated preoperative systemic inflammatory markers in localized soft tissue sarcoma.Cancer Biomark. 2016;16(3):333-42. doi: 10.3233/CBM-160571. Cancer Biomark. 2016. PMID: 26835589 Review.
Cited by
-
Development and validation of a risk prediction score for patients with nasopharyngeal carcinoma.Cancer Cell Int. 2021 Aug 26;21(1):452. doi: 10.1186/s12935-021-02158-6. Cancer Cell Int. 2021. PMID: 34446028 Free PMC article.
-
C-Reactive Protein as Predictive Biomarker for Response to Chemoradiotherapy in Patients with Locally Advanced Rectal Cancer: A Retrospective Study.Cancers (Basel). 2022 Jan 19;14(3):491. doi: 10.3390/cancers14030491. Cancers (Basel). 2022. PMID: 35158759 Free PMC article.
-
The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer.Diagnostics (Basel). 2023 Feb 11;13(4):679. doi: 10.3390/diagnostics13040679. Diagnostics (Basel). 2023. PMID: 36832166 Free PMC article.
-
No association between genetically predicted C-reactive protein levels and colorectal cancer survival in Korean: two-sample Mendelian randomization analysis.Epidemiol Health. 2023;45:e2023039. doi: 10.4178/epih.e2023039. Epub 2023 Mar 22. Epidemiol Health. 2023. PMID: 36996866 Free PMC article.
References
-
- Benson A.B., Venook A.P., Al-Hawary M.M., Cederquist L., Chen Y.J., Ciombor K.K., Cohen S., Cooper H.S., Deming D., Engstrom P.F., et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018;16:874–901. doi: 10.6004/jnccn.2018.0061. - DOI - PMC - PubMed
-
- Sauer R., Becker H., Hohenberger W., Rodel C., Wittekind C., Fietkau R., Martus P., Tschmelitsch J., Hager E., Hess C.F., et al. German Rectal Cancer Study, G., Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004;351:1731–1740. doi: 10.1056/NEJMoa040694. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
