

Baseline and Dynamic Risk Predictors of Appropriate Implantable Cardioverter Defibrillator Therapy
- PMID: 33023350
- PMCID: PMC7763383
- DOI: 10.1161/JAHA.120.017002
Baseline and Dynamic Risk Predictors of Appropriate Implantable Cardioverter Defibrillator Therapy
Abstract
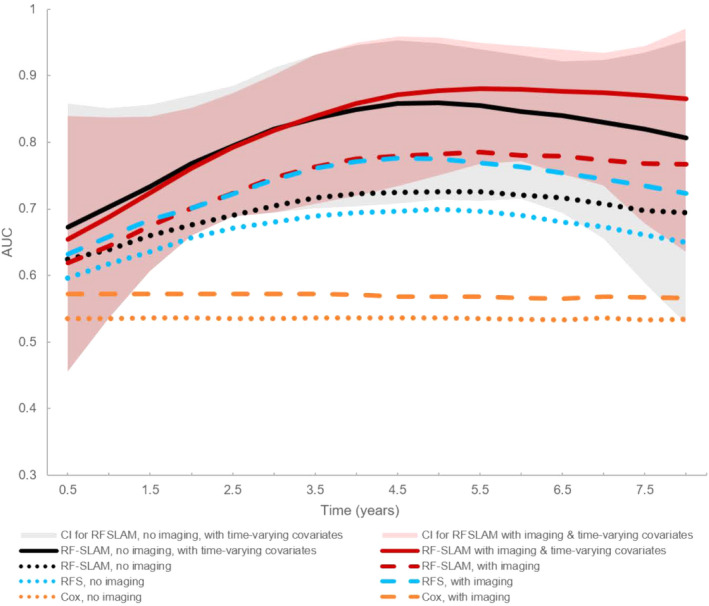
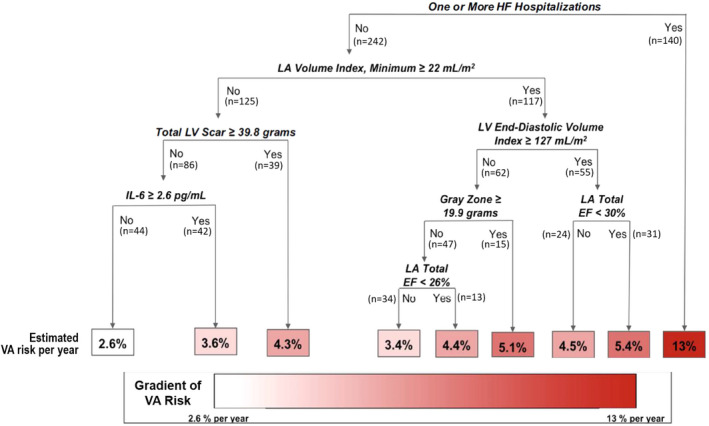
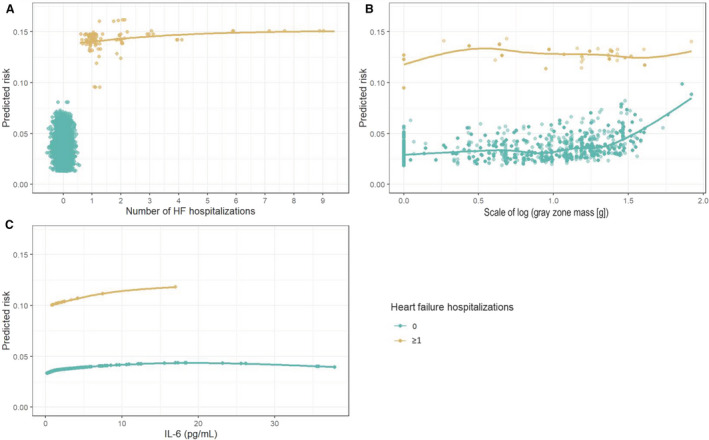
Background Current approaches fail to separate patients at high versus low risk for ventricular arrhythmias owing to overreliance on a snapshot left ventricular ejection fraction measure. We used statistical machine learning to identify important cardiac imaging and time-varying risk predictors. Methods and Results Three hundred eighty-two cardiomyopathy patients (left ventricular ejection fraction ≤35%) underwent cardiac magnetic resonance before primary prevention implantable cardioverter defibrillator insertion. The primary end point was appropriate implantable cardioverter defibrillator discharge or sudden death. Patient characteristics; serum biomarkers of inflammation, neurohormonal status, and injury; and cardiac magnetic resonance-measured left ventricle and left atrial indices and myocardial scar burden were assessed at baseline. Time-varying covariates comprised interval heart failure hospitalizations and left ventricular ejection fractions. A random forest statistical method for survival, longitudinal, and multivariable outcomes incorporating baseline and time-varying variables was compared with (1) Seattle Heart Failure model scores and (2) random forest survival and Cox regression models incorporating baseline characteristics with and without imaging variables. Age averaged 57±13 years with 28% women, 66% white, 51% ischemic, and follow-up time of 5.9±2.3 years. The primary end point (n=75) occurred at 3.3±2.4 years. Random forest statistical method for survival, longitudinal, and multivariable outcomes with baseline and time-varying predictors had the highest area under the receiver operating curve, median 0.88 (95% CI, 0.75-0.96). Top predictors comprised heart failure hospitalization, left ventricle scar, left ventricle and left atrial volumes, left atrial function, and interleukin-6 level; heart failure accounted for 67% of the variation explained by the prediction, imaging 27%, and interleukin-6 2%. Serial left ventricular ejection fraction was not a significant predictor. Conclusions Hospitalization for heart failure and baseline cardiac metrics substantially improve ventricular arrhythmic risk prediction.
Keywords: cardiac magnetic resonance imaging; heart failure; risk stratification; sudden cardiac death; ventricular arrhythmia.
Conflict of interest statement
None.
Figures
Comment in
-
Separating the Forest From the Trees: New Tools for a Personalized Sudden Cardiac Death Risk Stratification.J Am Heart Assoc. 2020 Oct 20;9(20):e018957. doi: 10.1161/JAHA.120.018957. Epub 2020 Oct 7. J Am Heart Assoc. 2020. PMID: 33025849 Free PMC article. No abstract available.
References
-
- Myerburg RJ, Goldberger JJ. Sudden cardiac arrest risk assessment: Population science and the individual risk mandate. JAMA Cardiol. 2017;2:689–694. - PubMed
-
- Greenlee RT, Go AS, Peterson PN, Cassidy‐Bushrow AE, Gaber C, Garcia‐Montilla R, Glenn KA, Gupta N, Gurwitz JH, Hammill SC, et al. Device therapies among patients receiving primary prevention implantable cardioverter‐defibrillators in the Cardiovascular research network. J Am Heart Assoc. 2018;7:e008292.DOI: 10.1161/JAHA.117.008292. - DOI - PMC - PubMed
-
- Sabbag A, Suleiman M, Laish‐Farkash A, Samania N, Kazatsker M, Goldenberg I, Glikson M, Beinart R. Contemporary rates of appropriate shock therapy in patients who receive implantable device therapy in a real‐world setting: From the Israeli ICD Registry. Heart Rhythm. 2015;12:2426–2433. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
