

Hermansky-Pudlak syndrome-associated pneumothorax with rapid progression of respiratory failure: a case report
- PMID: 33023548
- PMCID: PMC7541300
- DOI: 10.1186/s12890-020-01302-8
Hermansky-Pudlak syndrome-associated pneumothorax with rapid progression of respiratory failure: a case report
Abstract
Background: Hermansky-Pudlak syndrome (HPS) is an extremely rare disease with pulmonary fibrosis (PF), oculocutaneous albinism, induced platelet dysfunction, and granulomatous colitis. Although patients with HPS-associated PF (HPS-PF) often receive treatment with anti-fibrotic agents, including pirfenidone, many HPS-PF cases are progressive. The development of pneumothorax is known to be rare in HPS-PF. Pneumothorax development is generally important for prognosis in patients with interstitial pneumonia. However, there are few reports regarding the development of pneumothorax in patients with HPS-PF.
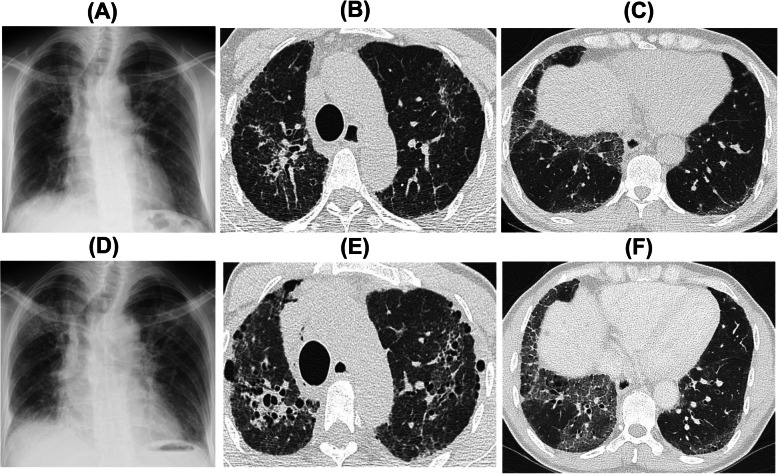
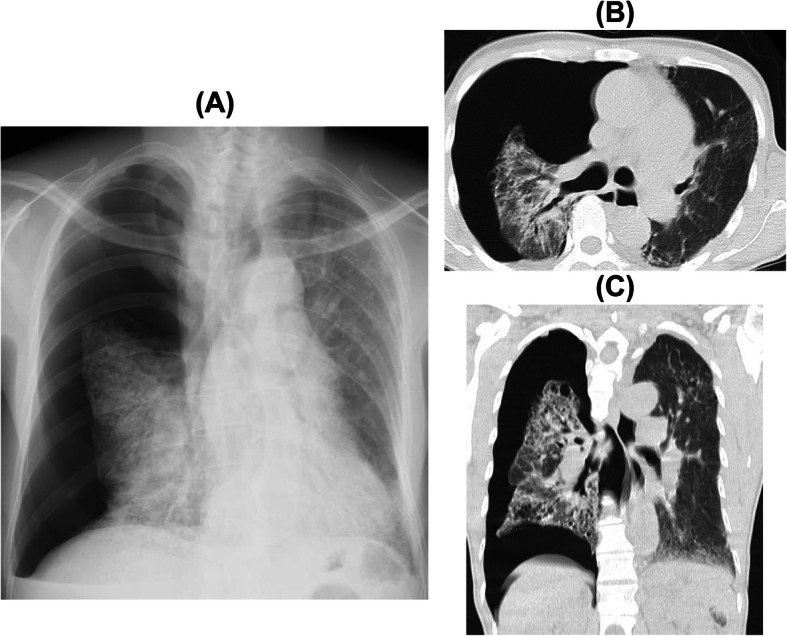
Case presentation: A 50-year-old Japanese man with chestnut hair, white skin, and light brown squint eyes visited our hospital for interstitial pneumonia examination. Chest high-resolution computed tomography (HRCT) demonstrated diffuse bilateral reticular opacities along the bronchovascular bundles and traction bronchiectasis predominantly in the upper lung fields. He was definitively diagnosed with HPS because genetic analysis showed that he had a homozygous mutation, c.398 + 5G > A, in the HPS-1 gene. After diagnosis with HPS-PF, he initiated home oxygen therapy due to gradually progressive hypoxemia. Three months after the HPS-PF diagnosis, the patient suddenly developed severe chest pain and dyspnea and was admitted to our hospital on emergency. He was diagnosed with pneumothorax by chest radiological findings. He immediately received chest drainage; however, his pneumothorax did not improve. Therefore, he underwent video-assisted surgery by thoracic surgeons. The leak point was not detected, but multiple bullae were found, mainly in the upper lung lobes. Thus, the surgeons did not perform bullectomy and only covered the apical areas. Fifteen days after the surgery, the patient developed high fever and dyspnea with a new diffuse reticular shadow found through HRCT. We first initiated the patient on broad-spectrum antibiotics; however, the symptoms and radiological findings worsened. Therefore, we started treatment with pirfenidone for inhibition of PF progression. The patient re-developed pneumothorax with severe respiratory failure. Although he re-underwent chest drainage, he died of progressive respiratory failure.
Conclusions: We herein report the case of a rare HPS patient who developed pneumothorax with progressive PF. Pneumothorax may cause rapid progressive respiratory failure and may be associated with PF progression in HPS-PF.
Keywords: Chest drainage; Hermansky-Pudlak syndrome; Pirfenidone; Pneumothorax; Pulmonary fibrosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
